Thomas F. Slaughter, MD, MHA, CPH
- Professor and Head, Section on Cardiothoracic Anesthesiology
- Wake Forest University School of Medicine
- Winston-Salem, North Carolina
It is the responsibility of caregivers/teachers to or older child is left alone with a child without another adult monitor what children are talking about and intervene when present (3 acne 4 weeks pregnant buy cheap eurax 20 gm online,4) skin care laser clinic birmingham generic 20gm eurax. Many instances have been reported where a child has Children like to test their skills and abilities acne on arms buy cheap eurax on-line. This is particu hidden when the group was moving to another location acne no more purchase genuine eurax online, larly noticeable around playground equipment acne 5 weeks pregnant purchase eurax line. Even if the or where the child wandered off when a door was opened highest safety standards for playground layout skin care careers order discount eurax line, design and for another purpose. Regular counting of children (name to surfacing are met, serious injuries can happen if children face) will alert the staff to begin a search before the child are left unsupervised. Adults who are involved, aware, and gets too far, into trouble, or slips into an unobserved loca appreciative of young childrens behaviors are in the best tion. Caregivers/teach b) Establishing clear and simple safety rules; ers should do the counts before the group leaves an area c) Being aware of and scanning for potential safety and when the group enters a new area. The facility should hazards; assign and reassign counting responsibility as needed to d) Placing yourself in a strategic position so you are maintain a counting routine. Facilities might consider count able to adapt to the needs of the child; ing systems such as using a reminder tone on a watch or e) Scanning play activities and circulating around the musical clock that sounds at timed intervals (about every area; ffteen minutes) to help the staff remember to count. Intl J Injury Control and Safety toilet, as well as monitor the bathroom to make sure that the Promotion 14:122-24. Public toilet facilities without direct visual observation but must playground safety handbook. Younger children who request privacy and have shown A child should not sit in a high chair or other equipment that capability to use toilet facilities properly should be given constrains his/her movement (1,2) indoors or outdoors for permission to use separate and private toilet facilities. Children should never be left out of the view and at Planning must include advance assignments, monitoring, tention of adult caregivers/teachers while in these types of and contingency plans to maintain appropriate staffng. A least restrictive environment should ing times when children are typically being dropped off and be encouraged at all times. Children should not be left to picked up, the number of children present can vary. Suffcient staff must be main tained to evacuate the children safely in case of emergency. They need opportunities to use and build sured by structured observation, by counting caregivers/ on their physical abilities. This is especially true for infants teachers and children in each group at varied times of the and toddlers who are eagerly using their bodies to explore day, and by reviewing written policies. University of Northern awake, restricting them to a seat may limit social interac Iowa. Department of Health and Human Reduction Services, Offce of the Assistant Secretary for Planning and Standard 5. Chapter 2: Program Activities 66 Caring for Our Children: National Health and Safety Performance Standards Finkelstein, K. Oxygen desaturation in term infants in than eight hours of television per week has been associ car safety seats. For children have higher intakes of sugar-sweetened beverage and lower two years and older in early care and early education set fruit and vegetable intakes (8). Children are exposed to tings, total screen time should be limited to not more than extensive advertising for high-calorie and low-nutrient dense thirty minutes once a week, and for educational or physi foods and drinks and very limited advertising of healthful cal activity use only. Computer use advertising infuences the food consumption of children should be limited to no more than ffteen-minute increments two-to eleven-years-old (9). Addition Parents/guardians should be informed if screen media are ally, young children engage in other forms of screen activity used in the early care and education program. Any screen several times a week or more including using a computer media used should be free of advertising and brand place (27%), playing console video games (13%), and playing ment. Interactive activities that promote brain differences between groups in the type of television content development can be encouraged, such as talking, playing, viewed, and in the proportions of programs in which no tele singing, and reading together. Associations between sedentary behavior appropriate books available for each cognitive stage of and blood pressure in young children. Arch Pediatric Adolescent Med Constant and active supervision should be maintained when 159:619-25. Pediatrics wading/water play activities where either an infant or a tod 124:1495-1503. Children ages thirteen months to fve years factors for obesity in childhood: Cohort study. British Medical J of age should not be permitted to play in areas where there 330:1357. Caregivers/teachers should ensure that all pools meet the Ethnicity and Disease 14:336-39. Association between television viewing and poor diet quality and spas to prevent underwater entrapment of children in in young children. Committee on Food Marketing and the Diets of Children and deaths of children of varying ages (2). The association of television In a comprehensive study of drowning and submersion in and video viewing with fast food intake by preschool-age children. Television viewing 77% of the victims had been missing from sight for and television in bedroom associated with overweight risk among fve minutes or less; low-income preschool children. Parents not occur to alert someone that the child is in trouble of preschoolers: Expert media recommendations and ratings (4). Drowning is the second leading cause of unintentional National Association for the Education of Young Children. Chapter 2: Program Activities 68 Caring for Our Children: National Health and Safety Performance Standards that examined where drowning most commonly takes place the need for constant supervision is of particular concern in concluded that infants are most likely to drown in bathtubs, dealing with very young children and children with signif toddlers are most likely to drown in swimming pools and cant motor dysfunction or developmental delays. Virginia Graeme Baker Pool and Spa Safety when riding on a boat or playing near a river, lake, Act. American Academy of Pediatrics, Committee on Injury, Violence, e) Teaching children never to swim alone or without and Poison Prevention. These rings usually contain HomeandRecreationalSafety/Water-Safety/waterinjuries three or four legs with suction cups that attach to the bot -factsheet. The suction cups, however, may release sud hazard with baby ?supporting ring devices. Infants and Thirty children under fve years of age died from drowning toddlers can drown in 5-gallon buckets: A hidden hazard in the in buckets, pails, and containers from 2003-2005 (10). American Academy of Pediatrics Committee on Injury, Violence, an adult should be watching them constantly. Technical report: Prevention ing adult should not read, play cards, talk on the telephone, of drowning. They should be taught that when going into a body of water, they 69 Chapter 2: Program Activities Caring for Our Children: National Health and Safety Performance Standards should go in feet frst the frst time to check the depth. Also such behavior can distract caregivers/teach interactions and engagement with others; ers from supervising other children, thereby placing the e) Modifying the learning/play environment. Department of Health and Human Services, Maternal and likely to know what to do and what is expected Child Health Bureau. A framework for teaching emergency lifesaving skills to children and When there is less anxiety, there may be less acting adolescents. The discipline standard clear encouragement and descriptive praise are used therefore refects an approach that focuses on preventing to give attention to appropriate behaviors, those behavior problems by supporting children in learning appro behaviors are likely to be repeated. For example, if a child has a encourage positive behavior and self regulation by hard time transitioning, the caregiver/teacher can Chapter 2: Program Activities 70 Caring for Our Children: National Health and Safety Performance Standards identify strategies to help the child with the transition teach new skills to replace the behavior. Listed below are (individualized warning, job during transition, guidelines when using time-out (8): individual schedule, peer buddy to help, etc. Time-out should only be used in time-out from positive enforcement; combination with instructional approaches that teach b) the caregiver/teacher should explain how time-out children what to do in place of the behavior problem. Discipline is most effective when it is supervision; consistent, reinforces desired behaviors, and offers natural e) Time-outs do not need to be long. Children have three minutes of time-out); to be taught expectations for their behavior if they are to f) the caregiver/teacher should end the time-out on a develop internal control of their actions. How to respond to failure to cooperate during time-out: On the contrary, children should not receive praise for unde Caregivers/teachers should expect resistance from children sirable behaviors, but instead be praised for honest efforts who are new to the time-out procedure. A comprehensive More resources for caregivers/teachers on discipline can behavior plan is often based frst on a positive, affectionate be found at the following organizations Websites: a) Center relationship between the child and the caregiver/teacher. Psychological be picked up and moved to another location in the room if Bulletin 128:774-95. Why the ?gentle smack should go: Policy invited to walk with you frst but, if not compliant, taken by review. Spanking by parents and subsequent with the child telling him/her the behavior is unacceptable. Arch Pediatric Adolescent Medicine the behavior persists, parents/guardians, caregivers/teach 151:761-67. Some consequences of early harsh might not have the social skills or language to communicate discipline: Child aggression and a maladaptive social information appropriately may use physical aggression to express them processing style. Department of Health and Human steps to deal with biting: Services, Offce of the Assistant Secretary for Planning and Step 1: If a child bites another child, the caregiver/teacher Evaluation. Promoting mental health in early childhood programs serving tions (available from the American Academy of Pediatrics families from low income neighborhoods. In Handbook of parent training: Helping parents prevent and solve Step 3: the caregiver/teacher should allow for ?dignity problem behaviors. Intrinsic and extrinsic motivation: the search for optimal motivation and performance, ed. Caregiver-child interactions and early literacy Caregivers/teachers need to consider why the child is biting development of preschool children from low-income environments. Suspension and other limita j) Lack of attention child receives attention when biting. He can get a wet paper towel, a blankie or favorite toy for the Child care programs should have a comprehensive disci victim and sit near them until the other child is feeling pline policy that includes an explicit description of alterna better. These Discussing aggressive behavior in group time with the chil policies should also explicitly state how the program plans dren can be an effective way to gain and share understand to use any available internal mental health and other sup ing among the children about how it feels when aggressive port staff during behavioral crises to eliminate to the degree behavior occurs. Although bullying has not been studied possible any need for external supports. Staff should have access to in-service training on both a proactive and as-needed basis on how to reduce the likeli For more helpful strategies for handling aggression, see hood of problem behaviors escalating to the level of risk for Center on the Social and Emotional Foundations for Early expulsion and how to more effectively manage behaviors Learning Website at csefel. Staff should also have a child care health consultant or child care mental health access to in-service training, resources, and child care consultant can help when the biting behavior continues. This transition could include a differ cess to such a consultant when more targeted child-specifc ent private or public-funded child care or early education interventions are needed. Mental health consultation may be program in the community that is better equipped to ad obtained from a variety of sources, as described in Standard dress the behavioral concerns. Prekindergarteners left behind: Expulsion j) Physical activity/outdoor time should not be taken rates in state prekindergarten programs. Preschool and child care clearly prohibited in family child care homes and centers in expulsion and suspension: Rates and predictors in one state. Implementing policies to reduce behavior problems in school (6,7), antisocial and criminal the likelihood of preschool expulsion. As infants become the following behaviors should be prohibited in all child care more mobile, the caregiver/teacher must create a safe settings and by all caregivers/teachers: space and impose limitations by encouraging activities that a) the use of corporal punishment. Brief verbal expres punishment means punishment inficted directly on sions of disapproval help prepare infants and toddlers for the body including, but not limited to: later use of reasoning. However, the caregiver/teacher 1) Hitting, spanking (refers to striking a child with an cannot expect infants and toddlers to be controlled by open hand on the buttocks or extremities with the verbal reprimands. Preschoolers have begun to develop an intention of modifying behavior without causing understanding of rules and can be expected to understand physical injury), shaking, slapping, twisting, ?time-out (out-of-group activity) under adult supervision as pulling, squeezing, or biting; a consequence for undesirable behavior. School-age chil 2) Demanding excessive physical exercise, excessive dren begin to develop a sense of personal responsibility and rest, or strenuous or bizarre postures; self-control and will recognize the removal of privileges (12). Children should not see hit b) Isolating a child in an adjacent room, hallway, closet, ting, ridicule, etc. Even though adults darkened area, play area, or any other area where a may state that the behaviors are ?playful, children cannot child cannot be seen or supervised; distinguish this. Warm, responsive touches convey a child; regard and concern for children of any age. Adults should g) Any abuse or maltreatment of a child, either as be sensitive to ensuring that their touches (such as pats on an incident of discipline or otherwise. Child care c) That such child restraint techniques do not violate the forms, licensed/ registered provider. Corporal punishment by parents and f) That a designated and trained staff person, who associated child behaviors and experiences: A meta-analytic and should be on the premises whenever this specifc theoretical review. Spanking by parents and subsequent fcation needs to be done after a restraining incident occurs antisocial behavior of children. Arch Pediatric Adolescent Medicine in order to conform with the mental health code. Physical removal discipline: Child aggression and a maladaptive social information of a child is defned according the development of the child. American Academy of Pediatrics, Committee on Psychological her to a quiet place where s/he cannot hurt themselves or Aspects of Child and Family Health. Prevention of child abuse in early childhood giving a lot of attention to the behavior, distracting the child programs and the responsibilities of early childhood professionals and/or giving a time-out to the child. Staff director annually to discuss how their child is doing in the should be alert to repeated instances of restraint for indi program. Effective responses: Caregivers/teachers should informally share with parents/ Physical restraint.

Using a toddler chang children in the room anti-acne buy eurax overnight delivery, do not rinse the soiled clothing ing table helps establish a well-organized changing area for in the toilet or elsewhere acne 9 month old purchase 20 gm eurax with amex. It is a good idea for the child care Caregivers/teachers should never leave a child unattended facility to request a few extra pair of socks and shoes on a table or countertop skin care clinique purchase eurax 20gm online, even for an instant acne on temples order eurax 20gm fast delivery. A safety strap from the parent/caregiver to be kept at the facility in or harness should not be used on the changing surface skin care addiction purchase cheap eurax online. Changing these undergarments can lead to risk for into the soiled pull-up or directly into a plastic-lined acne garret purchase eurax cheap online, spreading infection due to the contamination of surfaces hands-free covered can. The cover should with uncontaminated surfaces such as hands, furnishings, not require touching with contaminated hands or and foors (2,4). Posting the multi-step procedure may help objects; caregivers/teachers maintain the routine. Taking the supplies out of their containers and c) If gloves were used, remove them using the proper leaving the containers in their storage places reduces the technique (see Appendix D) and put them into a likelihood that the storage containers will become contami plastic-lined, hands-free covered can; nated during changing. Put the wipes paper that is large enough to cover the area likely to be into the plastic-lined, hands-free covered can. If the paper is large enough, there will be less need to remove visible soil from surfaces Step 4: Put on a clean pull-up or underwear and clothing, if later and there will be enough paper to fold up so the soiled necessary. Infectious organisms are present and detergent, rinse; on the skin and pull-ups or underwear even though they are d) Wet the entire changing surface with a disinfectant not seen. To reduce the contamination of clean surfaces, that is appropriate for the surface material you are caregivers/teachers should use a fresh wipe to wipe their treating. Although gloves may not Step 7: Perform hand hygiene according to the procedure in be required, they may provide a barrier against surface con Standard 3. Red book 2009: Report of the Committee on Infectious Prior to disinfecting the changing table, clean any visible Diseases. These soiling/wetting episodes can be due All staff, volunteers, and children should follow the proce to rapid onset gastroenteritis, distraction due to the intensity dure in Standard 3. These include new siblings, stress in the family, a) Upon arrival for the day, after breaks, or when or anxiety about changing classrooms or programs, all of moving from one child care group to another; which are based on their inability to recognize and articulate b) Before and after: their stress and to manage a variety of impulses. Even for preschool 5) Diapering; and kindergarten aged children, these accidents happen c) After: and these incidents are called ?accidents because of the 1) Using the toilet or helping a child use a toilet; frequency of these episodes among normally developing 2) Handling bodily fuid (mucus, blood, vomit), children. It is important for caregivers/teachers to recognize from sneezing, wiping and blowing noses, from that the need to assist young children with toileting is a mouths, or from sores; critical part of their work and that their attitude regarding the 3) Handling animals or cleaning up animal waste; incident and their support of children as they work toward 4) Playing in sand, on wooden play sets, and self regulation of their bodies is a component of teaching outdoors; young children. Effect of infection control measures on the many outbreaks of diarrhea among children and caregivers/ frequency of upper respiratory infection in child care: A randomized, teachers in child care centers (1). Proper handwashing promotes wellness In child care centers that have implemented hand hygiene in child care. Respiratory opportunities for the ingestion of zoonotic parasites that infections transmitted from animals. Infect Dis Clin North Am 5:649 could be present in contaminated sand and soil (6,7). Hand hygiene with Children and staff members should wash their hands using an alcohol-based sanitizer is an alternative to traditional the following method: handwashing with soap and water when visible soiling is not a) Check to be sure a clean, disposable paper (or present. Rub areas between f) In droplets of body fuids, such as those produced by fngers, around nail beds, under fngernails, jewelry, sneezing and coughing, that travel through the air. Association/American Academy of Pediatrics National health and Situations/times that children and staff should wash their safety guidelines for child-care programs; featured standards and hands should be posted in all handwashing areas. There are no data to support use of antibacterial handwashing and infection control in day-care centers. Douglas, 111 Chapter 3: Health Promotion Caring for Our Children: National Health and Safety Performance Standards Children and staff who need to open a door to leave a bath J Med 27:24-28. If a child can not open the door or turn off the faucet, Hand Hygiene they should be assisted by an adult. Wetting the hands before applying soap helps to create one arm and for children who can stand but not wash their a lather that can loosen soil. A child who can stand should either and brings it into solution on the surface of the skin. After assisting the child with handwashing, the staff 60?F and 120?F, is more comfortable than cold water; using member should wash his or her own hands. Hand hygiene warm water also promotes adequate rinsing during hand with an alcohol-based sanitizer is an alternative to hand washing (1). A ?how When running water is unavailable or impractical, the use of to poster that is developmentally appropriate should be alcohol-based hand sanitizer (Standard 3. For examples of handwashing posters, see: Outbreaks of disease have been linked to shared wash California Childcare Health Program at water and wash basins (4). Camp sinks and portable North Carolina Child Care Health and Safety Resource Cen commercial sinks with foot or hand pumps dispense water ter at. The staff should clean and disinfect the water reservoir container and water catch basin daily. Preventing tion of towel; and the spread of infuenza (the fu) in child care settings: Guidance for b) Incidents of unintentional strangulation have been administrators, caregivers/teachers, and other staff. Effect of infection control measures on the electrical outlets; frequency of upper respiratory infection in child care: A randomized, g) Wall mounted dispensers installed directly over controlled trial. Handwashing to carpeted foors should be permitted only in child care prevent diarrhea in day care centers. Effect of infection control measures on the alcohol-based hand sanitizer after washing hands with soap frequency of diarrheal episodes in child care: A randomized, and water is effective in reducing illness transmission in controlled trial. Hand sanitizer products may be dangerous or toxic if infections in toddlers attending daycare centers. As with any hand hygiene product, supervision of care health consultation improves health and safety policies and children is required to monitor effective use and to avoid practices. Acta ***Addition to Related Standards in second printing, August 2011 113 Chapter 3: Health Promotion Caring for Our Children: National Health and Safety Performance Standards Paediatrica 97:1672-80. Department of Health and Human Services, Centers for downloadable posters and fyers in multiple languages, go Disease Control and Prevention. The caregiver/teacher If nasal bulb syringes are used, facilities should have a writ should wear gloves if there is contact with any wound (cut ten policy that indicates: or scrape) that has material that could be transmitted to a) Rationale and protocols for use of nasal bulb another surface. Staff members and children should be taught to cover their mouths and noses with a tissue when they cough or sneeze. Caregivers/teachers tions should be used to handle potential exposure to blood, should consult with local health departments for including blood-containing body fuids and tissue discharg additional guidance on cleaning contaminated es, and to handle other potentially infectious fuids. In child care settings: Prior to using a disinfectant, clean the surface with a de a) Use of disposable gloves is optional unless blood tergent and rinse well with water. For guidance on disinfectants, refer to Ap cleaning up of spills of human milk, or for diapering; pendix J, Selecting an Appropriate Sanitizer or Disinfectant. Flush moisture-resistant disposable diaper table paper, the exposed area thoroughly with water. Training must comply with require membrane(s) exposures to toxic substances is to fush the ments of the Occupational Safety and Health Administration affected area for at least ffteen to twenty minutes. Bacteria and vi infectious body fuids and tissue discharges; and ruses carried in the blood, such as hepatitis B, pose a small 2) Reduce the spread of infectious material within but specifc risk in the child care setting (3). In addition, are disinfected before further contact occurs with hepatitis B virus can survive in a dried state in the environ them by other objects or individuals. Care infectious diseases without having symptoms, and many are should be taken and eye protection used to avoid contagious before they experience a symptom, staff mem splashing any contaminated materials onto any bers need to protect themselves and the children they serve mucus membrane (eyes, nose, mouth); by adhering to Standard Precautions for all activities. While human milk can be 115 Chapter 3: Health Promotion Caring for Our Children: National Health and Safety Performance Standards contaminated with blood from a cracked nipple, the risk of c) Use appropriate work practices to reduce the chance transmission of infection to caregivers/teachers who are of reactions to latex; feeding expressed human milk is almost negligible and this d) When wearing latex gloves, do not use oil-based represents a theoretical risk. Wearing of gloves to feed or hand creams or lotions (which can cause glove clean up spills of expressed human milk is unnecessary, but deterioration); caregivers/teachers should avoid getting expressed human e) After removing latex gloves, wash hands with a mild milk on their hands, if they have any open skin or sores on soap and dry thoroughly; their hands. If caregivers/teachers have open wounds they f) Practice good housekeeping, frequently clean areas should be protected by waterproof bandages or disposable and equipment contaminated with latex-containing gloves. Extracting as latex allergy; much of the contaminating material as possible before it h) Learn to recognize the symptoms of latex allergy: penetrates the surface to lower layers helps to minimize this skin rash; hives; fushing; itching; nasal, eye, or sinus challenge. Cleaning and disinfecting the surface without symptoms; asthma; and (rarely) shock. Either single-use disposable gloves or utility gloves should be used when disinfecting. The wearing of gloves Diseases does not prevent contamination of hands or of surfaces Appendix D: Gloving touched with contaminated gloved hands. Hand hygiene Appendix J: Selecting an Appropriate Sanitizer or Disinfectant Appendix L: Cleaning Up Body Fluids and sanitizing of contaminated surfaces is required when gloves are used. Latex allergy in children: tions in both the individual wearing the latex glove and the Modalities and prevention. Hand-washing and a) Use non-latex gloves for activities that are not likely diapering equipment reduces disease among children in out-of to involve contact with infectious materials (food home child care centers. Center for b) Use appropriate barrier protection when handling Disease Control and Prevention. Creating a contact dermatitis); Chapter 3: Health Promotion 116 Caring for Our Children: National Health and Safety Performance Standards latex-safe school for latex-sensitive children. Bacterial spores are dormant bacteria that have formed a protective shell, Keeping objects and surfaces in a child care setting as enabling them to survive extreme conditions for years. The clean and free of pathogens as possible requires a combi spores reactivate after entry into a host (such as a person), nation of: where conditions are favorable for them to live and repro a) Frequent cleaning; and duce (6). It is important to use the least toxic cleaner, sanitizer used in close proximity to children, and adequate ventila and disinfectant for the particular job. Products must be used according to manu teachers from inhaling potentially toxic fumes. Sanitize safely and a ?frst step because the purpose of the bleach and water effectively: Bleach and alternatives in child care programs. Health solution is to sanitize (it is not designed to clean and is not and Safety Notes (July). Infectious diarrhoea in children: surface with water, should occur before spraying the surface Controlling transmission in the child care setting. Prevalence of Each term has a specifc purpose and there are many meth rotavirus on high-risk fomites in day-care facilities. These toys should be laundered before Bedding (sheets, pillows, blankets, sleeping bags) should be being used by another child. All toys can and the mats or cots are taken out of storage during nap spread disease when children put the toys in their mouths, time, and then placed back in storage. Providing bedding touch the toys after putting their hands in their mouths dur for each child and storing each set in individually labeled ing play or eating, or after toileting with inadequate hand bins, cubbies, or bags in a manner that separates the hygiene. Using a mechanical dishwasher is an acceptable personal articles of one individual from those of another are labor-saving approach for sanitizing plastic toys as long appropriate hygienic practices (1). Red book: 2009 report of the Committee on Infectious enough toys to rotate through cleaning makes this method Diseases, 153. Respiratory Tobacco use, alcohol, and illegal drugs should be prohibited effects of environmental tobacco smoke in a panel study of on the premises of the program (both indoor and outdoor asthmatic and symptomatic children. Am J Resp Crit Care Med environments) and in any vehicles used by the program at 161:802-6. Infants and young of environmental tobacco smoke exposure on the respiratory health children exposed to secondhand smoke are at risk of de of children 2 months through 5 years of age in the United States: veloping bronchitis, pneumonia, and middle ear infections Third national health and nutritional examination survey, 1988 to when they experience common respiratory infections (1-5). Beliefs about the health effects space does not eliminate or minimize exposure of nonsmok of ?thirdhand smoke and home smoking bans. Progress towards a fre-safe ticles clinging to smokers hair and clothing, cushions and cigarette. The residue includes heavy metals, carcino smoking and alcohol drinking with residential fre injuries. Am J gens and radioactive materials that young children can get Epidemiol 135:26-34. Safe d) Rabbit; child care necessitates alert, unimpaired caregivers/teach e) Rodent. The use of alcoholic beverages in family child care homes Fish are permissible but must be inaccessible to children. Drugs, and Toxic Substances 119 Chapter 3: Health Promotion Caring for Our Children: National Health and Safety Performance Standards Only animals that do not pose a health or safety risk will be Special precautions may be needed to minimize the risk of allowed on the premises of the facility. The caregiver/teacher should instruct children on the hu When animals are taken out of their natural environment and mane and safe procedures to follow when in close proximity are in situations unusual to them, the stress that the animals to animals (for example, not to provoke or startle animals or experience may cause them to act aggressively or attempt touch them when they are near food). Appropriate re straint devices will allow the holder to react quickly, prevent All contact between animals and children should be super harm to children and/or the escape of the animal (9). Children should not be allowed to feed animals directly from Toxoplasmosis can cause problems with pregnancy, includ their hands. Animals teach children about how protects them from competition by other animals while be to be gentle and responsible, about life and death, and ing fed which would also provide protection for the children about unconditional love (9). Cleaning air flters more often if animals are in Children should be discouraged from ?kissing animals or childcare areas may be helpful in reducing animal dander. Some dogs complete training and are certifed as part of All children and caregivers/teachers who handle animals or ?dog-assisted therapy programs. For in place that specifes if there are precautionary measures to more information on this program and resources, contact be taken before the child has direct or indirect contact with Therapy Dogs International at. Effects of gender and parental the facility and when visiting a zoo or local pet store (5,9,10). Compendium of measures to prevent disease associated with animals in public settings. Department Chapter 3: Health Promotion 120 Caring for Our Children: National Health and Safety Performance Standards of Health and Human Services, Centers for Disease Control and i) Psittacine birds unless tested for psittacosis Prevention. Appendix D: Guidelines for animals in school and Inclusive of parrots, parakeets, budgies, and child-care settings. Department of Health and Human Services, Centers for can be transferred to humans; Disease Control and Prevention.
Other spaces skin care lines purchase eurax 20 gm fast delivery, like block areas skin care yang bagus dan murah buy eurax paypal, can be larger because the nature of the play can handle a larger group acne xarelto buy eurax 20gm on line. Designate areas for quiet play (like puzzles) by taking advantage of cozy spaces or adding carpet or pillows to absorb sound acne 24 order eurax in united states online. Likewise acne icd 10 eurax 20gm on-line, designate space for more active play (dramatic play acne necrotica cheap 20 gm eurax mastercard, puppets, obstacle course) so that children have a variety of play experiences during the day. Be sure that the kinds of materials and the physical arrangement of the play spaces clearly give children the message of active versus quiet play and that the two areas are distinct and separate. Use the physical arrangement of space to suggest play activities and give children cues that define the play you expect in that space. For example, if blocks are stored in a box without a clearly defined space for block play, it is likely that children will not see how to use these materials appropriately. Family Child Care Homes In family child care homes the environment the children use is typically the same as the family that lives in the home. A major reason that parents choose family child care is because they want their child in a home ?like environment. There is a balance that family child care providers must reach when running their programs. Below are some factors to consider when thinking about your family child care environment. They must be careful to close cabinets in the kitchen and close doors to other areas of the home that children should not have access too. Always consider your ability to safely supervise and monitor children in your care. Pay particular attention to supporting the needs of your youngest children as well as enhancing the activities of those children that are older. Create a Child Sanctuary A child sanctuary is a small, semi enclosed space with room for only one or two children. The space should be visually isolated from other children but easily supervised by adults. When children are having a difficult time they might need a space for some privacy or to limit their contact with others. We must make a special effort to teach children how to take breaks and to pace their interactions. Well-designed private spaces can provide children with a safe refuge to re-focus their energy and gain self control. Management of the Child Sanctuary To effectively manage the child sanctuary make sure that the rules are clearly defined and that all the adults understand the purpose of the private space. Teach children the strategies for politely telling another person that they do not wish to be disturbed when they are in the child sanctuary. Always remember that the child sanctuary is a place for refuge and re-grouping and should never be used as a timeout/punishment area. Create Attractive, Sensory-Rich Activity Areas Many early childhood professionals do a good job of adding interesting items to the play space, but it is also important to weed out items that have served their purpose. Eliminating clutter helps children focus on new material while decreasing the number of stimuli to which they must attend. The list below highlights several low cost and practical ways to improve upon a focused centers environment: Y Modify the lighting in the space. Y Install dimmer switches to control the intensity of the lighting different sections of the room. Y Modify ceiling height or floor level when possible to create spaces that are cozy, nurturing and child sized for comfort. Y Define an activity area by draping strips of cloth across and between dowel rods hung from the ceiling. This strategy softens and area of the room and actually makes the ceiling appears to be lower and is especially useful when a private, quiet, semi-enclosed activity area is desired Y Make rooms pleasant and attractive by creating visual, auditory, olfactory, and textural interest. Y Carpet bare floors; cover bulletin boards with cork or burlap, or hang large collages made from cloth or other materials. Y Create a touch wall as an activity with the children to learn about various textures and materials. Having Enough Materials Young children are more likely to get involved in play when there is plenty of fun, challenging, and intriguing play materials. It is important to include a range of activities and toys for children of different ages and abilities. It is also important to include enough materials to successfully engage all the chidlren. Children who fully engage in intriguing play activities require less adult intervention and are less likely to display inappropriate behaviors. Y It is easier for group of children to play together when there are multiples of the same items. It is not developmentally appropriate to expect very young children to share toys or other favorite materials. Y Consider the number and ages of children in the program when deciding how many types of activity areas to include. Y Arrange your space so that there is one-third more activity space than children, to allow children movement from one activity to another without waiting. Schedule Enough Time In addition to having enough materials, young children need extended periods of play that are not interrupted by demands to hurry, clean up, or give someone else a turn. Instead, their energy becomes focused on, ?grabbing enough stuff, being the first in line, or refusing to get off the swing. Y Regularly schedule routines like mealtimes, outdoor play, or even going home sometimes make it impossible for child to finish an activity. For example, allow the paint easel to stay up until the next morning or put a play-dough sculpture in an airtight container until later in the day. Y Allow the child to tell you when a particular project or some structure is completed. If, for example, a child wants to add to a picture hung on the wall, be sure that she has the opportunity to make additions or changes. Y Asking a child to play for five minutes with the toys so that someone else can take it away is not an effective way of setting up a successful schedule. Plan Smooth Transitions Many challenging behaviors occur during transitions from one activity to the next. Even when children have had plenty of time to play, it is difficult for them to move on to another activity. Young children benefit from a schedule that requires a limited number of transitions throughout the day. When a transition is necessary, it should be well-planned to allow enough time for children to participate at their own pace. The following suggestions provide children with tools to understand routine and direct their own behavior during transitions. For example, children might naturally move to put on coats after lunch if outdoor play routinely follows lunch. You might use actual photographs of your play yard, lunch table, and play centers in sequential order or draw pictures to represent different parts of your day. Y Whenever possible, give children advance notice if the schedule is going to change. Make Waiting Time Productive Scheduling a time when children have nothing to do but wait is asking them to invent something to do-often something you wish they would not do! Standing in line to go outside, sitting idly at the table while others finish snack or waiting in line to wash hands are common examples of unnecessary waiting. Young children will fidget, move around, and find ways to interact with the person next to them to pass the time. This kind of play is part of their communication and expression and it is appropriate. In fact, when two or more activities take place at the same time, no one has to wait their turn and the smaller groups promote better learning. If snack is prepared and placed on the table, children can wash their hands and come to snack as they finish playing without waiting in line. If one adult helps some of the children begin a painting activity and the other stays with children who are still involved in other play areas, no one has to wait. Y If staff are alone with children, they could set up a few child-directed activities close enough in proximity to supervise. While waiting for the bus, encourage children to sing, count the cars going by, or tell stories. The Origins of Intelligence in Children: New York International Universities Press. Spaces for Children: the Build Environment and Child Development, NewYork: Plenum Press, 1987. Jhalak Gautam (Ministry of Health and Population) for their thorough and insightful reviews that helped improve the clarity and quality of this report. Recommended citation: Singh, Samikshya, Gambhir Shrestha, Deepak Joshi, and Tesfayi Gebreselassie. The standard format of the survey final report included only a descriptive presentation of findings and trends, and did not include analytical methods that can ascertain the significance of change and association among variables. Although largely sufficient, the final report is limited, particularly in providing answers to ?why answers that are essential in reshaping important policies and programs. This information provides guidance for planning, implementing, refocusing, monitoring, and evaluating health programs in Nepal. The long term objective of the further analysis is to strengthen the technical capacity of local institutions and individuals for analyzing and using data from complex national population and health surveys to better understand specific issues related to country need. The participation and cooperation of the members of the Technical Advisory Committee in the different phases of the survey are highly valued. I would like to express my deep appreciation for the contributions of many different stakeholders and for their valuable input in the various phases of the study and the final report. However, children from poor households were less likely to seek treatment or advice from health facilities or providers. Reductions in neonatal and under-5 mortality were documented in Nepal over the decade. In addition, multivariate analysis showed that smaller neonates and neonates who were not weighed at the time of birth were more likely to die in the neonatal period, while neonates born in Province 1 had a lower likelihood of dying compared to those from Province 7 (Sudurpashchim Province). For under-5 children, those who had not received immediate newborn care were more likely to die before their fifth birthday. In addition, a 2016 epidemiological study found that diarrhea prevalence was higher among nonexclusively-breastfed children under 6 months of age, children of a nonformal working father, and children from a community where there were other children with diarrhea (Kalakheti, Panthee, and Jain 2016). A study conducted in Dhulikhel hospital in 2014 found that an unclean cooking stove (smoked cooking stove) and parental smoking were significant determinants of pneumonia in under-5 children (Karki, Fitzpatrick, and Shrestha 2014). A multi-country study of Sub-Saharan Africa also revealed that children from wealthier households, a household with an improved toilet, and children who were protected against fever-related diseases were less likely to have a fever (Novignon and Nonvignon 2012). A study conducted in Lalitpur, Nepal, on the health-seeking behavior of mothers of sick children found that a significantly higher proportion of mothers with primary or higher education, male children, and children experiencing pneumonia sought treatment or advice from health facilities or providers (Shrestha 2015). Findings from a case-control study conducted in Chitwan, Nepal, showed that low birth weight, applying nothing on the cord, not wrapping the newborn immediately after birth, and neonates of women with no formal schooling were more likely to die during the neonatal period (Shah et al. Similarly, female children, wanted births, and children of parents with some education had a lower risk of dying before completing their fifth birthday, while children of working women, tobacco smoking/chewing women, and women who were not using contraceptives had a higher risk of under-5 deaths (Sohail 2017). Nepal has targeted the reduction of under-5 mortality to 28 per 1,000 live births and the neonatal mortality rate to 12 per 1,000 live births by 2030 (MoH 2016; National Planning Commission 2017). Even more challenging is the goal of reducing neonatal mortality to below 12 per 1,000 live births from the current rate of 21 per 1,000 live births. Few studies were conducted to better understand the predictors of childhood illnesses, childhood treatment seeking practices, and mortality by using nationally representative data. In addition, the analysis found no difference in receiving 3 treatment from government-owned health facilities by various characteristics (Quinley and Govindasamy 2007). Nepal has undergone a political, administrative, social, and economic transformation in the last decade, as well as changes in disease prevalence, treatment-seeking behavior, and mortality. As a result, the determinants in 2006 or 2011 may not be the same as those in 2016. The findings are expected to help policymakers design interventions that further reduce newborn and under-5 deaths and disease prevalence, and also improve treatment or advice-seeking practices. The conceptual framework below (Figure 1) was based on a literature review and consultations with experts from government agencies, nongovernment organizations, and academia. The surveys included a nationally representative sample of women age 15-49 who also provided information on their birth histories and child health in the last 5 years preceding the survey. This report presents further analysis of the prevalence of childhood illnesses, their treatment or advice-seeking practices from health facilities or other providers, and childhood mortality. A total of 10,150 live births in the 10 years before the survey were used to estimate neonatal and under-5 mortality rate for all variables except the maternal service use variables. All births that occurred in the previous 5 years (5,007 live births) were used to estimate mortality rates by place of delivery, while mortality rates for antenatal care and immediate newborn care were estimated from 3,935 live births (last births in the previous 5 years only). A total of 269 children died in the neonatal period, while 435 children died before their fifth birthday in the 10 years before the survey. In the calculation of the neonatal and under-5 mortality, a total of 3,935 live births (last births) in the 5 years before the survey were used. Trend analysis is used to observe changes in the six outcome indicators over a 10-year period (2006 and 2016). The association between predictors (independent variables) and the outcome variable was evaluated using a chi-square test (bivariate analysis).
Tose children ages three and pea-sized amount for children ages three years of age and older should use a pea-sized amount of fuoride toothpaste older (1) acne under jawline purchase 20gm eurax fast delivery. Disposable gloves toothpaste is the most efcient way to apply fuoride to the should be worn by the caregiver/teacher if contact with a teeth skin care routine 20 gm eurax for sale. The care caused by over exposure to fuoride during the frst eight giver/teacher should monitor the tooth brushing activity years of life (5) acne yellow crust buy eurax 20 gm without a prescription. The children can rinse with water afer a snack or a meal if Children whose teeth are properly brushed with fuoride their teeth have been brushed with fuoride toothpaste toothpaste at home twice a day and are at low risk for earlier acne refresh 080 cheap eurax 20gm on-line. Each child can use a cup of water for tooth The cavity-causing efect of exposure to foods or drinks brushing acne 911 eurax 20 gm with mastercard. The child should wet the brush in the cup acne 6 days before period generic 20 gm eurax with visa, brush containing sugar (like juice) may be reduced by having chil and then spit excess toothpaste into the cup. Tere is currently no (strong) evidence of oral health care delivered in a comprehensive, continu that shows any beneft to wiping the gums of a baby who ously accessible, coordinated and family-centered way. Good oral hygiene is as important for a during well child care in this population while promoting six-month-old child with one tooth as it is for a six-year-old the establishment of a dental home (2). Tooth brushing with fuoride 109 Chapter 3: Health Promotion and Protection Fluoride varnish applied to all children every 3-6 months at 3. Coupled should have a personally labeled, sof toothbrush of age-ap with parent/guardian and caregiver/teacher education, propriate size. Guideline on periodicity of Photo Credit: National Center on Early Childhood Health and Wellness examination, preventive dental services, anticipatory guidance/ counseling, and oral treatment for infants, children, and adolescents. Some bleeding may occur perspective on physicians or other non-dental providers applying fuoride varnish. Some risk of infection can occur when numerous children Adolescent children should be informed about the efect brush their teeth and spit into the sink that is not sanitized of tobacco products on their oral health and additional between uses. Adults helping children brush their teeth not or moisten it or share a toothbrush with a child due to the only help them learn how to brush, but also improve the risk of promoting early colonization of the infant oral removal of plaque and food debris from all teeth (5). Information on what plaque is; developed by the National Resource Center for Health and b. American Academy of Pediatric Dentistry, Clinical Afairs Committee, Council on Clinical Afairs. Guideline on periodicity of Terefore, single-use disposable diapers should be examination, preventive dental services, anticipatory guidance/counseling, encouraged for use in child care facilities. Gastrointestinal tract disease, or diarrhea (caused by Policy statement: Oral health risk assessment timing and establishment of the dental home. Protective procedures includes minimal handling of soiled diapers and clothing, thorough hand hygiene, and containment of fecal matter. Diapering practices that reduce the frequency and Facilities should adhere to the procedures outlined in severity of diaper dermatitis will require less application of 3. The action and stool and minimize exposure to human waste in the of fecal digestive enzymes on urinary urea and the resulting child care setting. Children should use disposable diapers production of ammonia make the diapered area more alka with absorbent material. Damaged Cloth diapers should have an absorbent inner layer that is skin is more susceptible to other biological, chemical, and completely covered with an outer waterproof layer that has physical insults that can cause or aggravate diaper dermati a waist closure. Modern disposable diapered area more alkaline, which has been shown to diaper constructions: Innovations in performance help maintain healthy diapered skin. Putting stool into a Underwear/Pull-Ups and Clothing toilet in the child care facility increases the likelihood that 3. The signage should be front to back and use a fresh wipe, or a dampened cloth simple and should be in multiple languages if caregivers/ or wet paper towel each time you swipe. All employees who will diaper should undergo into a plastic-lined, hands-free covered can. Put soiled clothes in a plastic-lined, hands-free plastic bag; Step 1: Get organized. Note and plan to report any skin problems such as clothing away from you and any surfaces you cannot easily redness, skin cracks, or bleeding; clean and sanitize afer the change. Always keep a hand on the child; between the child and the diaper when inserting the pin. If clothing was soiled, securely tie the plastic bag used of organisms carried into the environment in this way. Remove any visible soil from the changing surface with even though they are not seen. This Step 8: Perform hand hygiene according to the procedure in may reduce the presence of enteric pathogens under the Standard 3. To achieve maximum beneft from use of blood in the stool, or any skin irritation), and report gloves, the caregiver/teacher must remove the gloves prop as necessary (2). Terefore safety straps on diaper tainers and leaving the containers in their storage places changing surfaces are not recommended. Caregivers/teachers as part of staf evaluation of caregivers/teachers who change can also use plastic clothes pins that can be washed and pull-ups or underwear and clothing. The signage should be sanitized to keep the clothing out of the way; simple and should be in multiple languages if caregivers/ c. All employees who will underwear is being changed, remove the soiled under change pull-ups or underwear and clothing should undergo wear and any soiled clothing, doing your best to avoid training and periodic assessment of these practices. Changing tables 116 Caring for Our Children: National Health and Safety Performance Standards. Remove stool and undergarments can lead to risk for spreading infection due urine from front to back and use a fresh wipe, damp to the contamination of surfaces from urine or feces (1). Taking the supplies out of their containers fold over the soiled area so a fresh, unsoiled paper and leaving the containers in their storage places reduces surface is now under the child; the likelihood that the storage containers will become c. Put the wipes into will be less need to remove visible soil from surfaces later the plastic-lined, hands-free covered can; and there will be enough paper to fold up so the soiled surface is not in contact with clean surfaces while dressing Step 4: Put on a clean pull-up or underwear and clothing, if the child. To reduce the contamination of clean to store the clothing and send home; surfaces, caregivers/teachers should use a fresh wipe to c. Remove any visible soil from the changing surface wipe their hands afer removing the gloves or, if no gloves with a disposable paper towel saturated with water were used, before proceeding to handle the clean pull-up or and detergent, rinse; underwear and the clothing. This may may require rinsing the change table surface with fresh reduce the presence of enteric pathogens under the water aferwards. Terefore, the spray and Disinfecting bottle should be put away before hand hygiene is performed (the last and essential part of every change) (6). It is important for caregivers/teachers to recognize that the need to assist young children with toileting is a critical part of their work and that their attitude regarding the incident and their support of children as they work 118 Caring for Our Children: National Health and Safety Performance Standards sanitizer is an alternative to traditional handwashing with 3. In body fuids (saliva, nasal discharge, secretions from cuts, or scrapes) may be encountered; open injuries; eye discharge, blood); 4. Handling bodily fuid (mucus, blood, vomit), from sneezing, wiping and blowing noses, from mouths, Since many infected people carry infectious organisms or from sores; without symptoms and many are contagious before they 3. Playing in sand, on wooden play sets, and outdoors; hygiene is the safest practice (1). Managing infectious diseases in child care and schools: A quick reference guide, 4 th Edition. In: Red book: 2015 report of the committee on removes organisms from the skin and allows them to be infectious diseases. Zoonoses: Biology, Children and staf who need to open a door to leave a bath clinical practice, and public health control. Handwashing: Clean disposable towel to avoid possibly re-contaminating clean hands save lives. Turn on clean, running water to a comfortable are the age group at greatest risk of spreading diarrheal temperature (1); disease due to frequent diaper changing. However, while hand sanitizers are terial) to hands; not recommended for children under the age of 2, they are d. Rub areas between fngers, around nail beds, Pre-moistened cleansing towelettes do not efectively clean under fngernails, jewelry, and back of hands. Leave the water running while drying hands; Outbreaks of disease have been linked to shared wash f. Dry hands with the clean, disposable paper or single use water and wash basins (7). The use of alcohol based hand sanitizers is an alternative to traditional handwashing (with soap and water) if soap and The use of cloth roller towels is not recommended because water is not available and if hands are not visibly dirty (4,5). Appendix K: Routine Schedule for Cleaning, Sanitizing, Use of antimicrobial soap is not recommended in child care and Disinfecting settings. Managing infectious diseases in child care and other cleaning procedures can reduce the occurrence and schools: A quick reference guide. Show me the science-When and how to use hand shown to reduce transmission of organisms that cause sanitizer. Efect of infection control measures on the frequency of upper respiratory infection in child care: A randomized, controlled trial. Handwashing to prevent handwashing with soap and water by children over twen diarrhea in day care centers. Diarrheal illness among infants and toddlers in day that is developmentally appropriate should be placed wher care centers: Efects of active surveillance and staf training without ever children wash their hands. Tese germs are Hand sanitizers using an alcohol-based active ingredient common in child care settings, and children less than 2 must contain 60% to 95% alcohol to be efective in killing years are at the greatest risk of spreading diarrheal disease most germs including multi-drug resistant pathogens. Some hand sanitizing products contain non-alcohol and Where alcohol-based hand sanitizer dispensers are used: ?natural ingredients. Show me the science-When and how to use or adjacent to ignition sources such as electrical outlets; hand sanitizer. Reported When alcohol based hand sanitizers are ofered in a child adverse health efects in children from ingestion of alcohol-based hand sanitizers United States, 2011?2014. Studies have demonstrated that using an alcohol-based Summaries of Infectious Diseases. Department of Health and Human Services, Centers for Disease ingested in amounts greater than the residue lef on hands Control and Prevention. Nasal bulb syringes should be cleaned with warm soapy teacher should wear gloves if there is contact with any water and stored open to air. Floors, rugs, and carpeting that have been contami and Body Fluids nated by body fuids should be cleaned by blotting Child care facilities should adopt the use of Standard to remove the fuid as quickly as possible, then disin Precautions developed for use in hospitals by The Centers fected by spot-cleaning with a detergent-disinfectant. The optimal length of borne pathogens before beginning to work in the facility time for washing or fushing an exposed area is not known. Reduce the spread of infectious material within the as hepatitis B, pose a small but specifc risk in the child care child care facility. Some other body fuids such as saliva contaminated nasal discharge, eye discharge, injury or tissue dis with blood or blood-associated fuids may contain live virus charges occur, these spills should be cleaned up (such as hepatitis B virus) but at lower concentrations than are immediately, and further managed as follows: found in blood itself. When wearing latex gloves, do not use oil-based hand expressed human milk is unnecessary, but caregivers/ creams or lotions (which can cause glove deterioration); teachers should avoid getting expressed human milk on. Practice good housekeeping, frequently clean areas and be protected by waterproof bandages or disposable gloves. Extracting and become familiar with procedures for preventing as much of the contaminating material as possible before it latex allergy; penetrates the surface to lower layers helps to minimize this h. Terefore, alternatives Natural fngernails that are long or wearing artifcial fnger to the use of carpeting and rugs are favored in the child nails or extenders is not recommended. The wearing of gloves Diseases does not prevent contamination of hands or of surfaces Appendix D: Gloving touched with contaminated gloved hands. Hand hygiene and sanitizing of contaminated surfaces is required when Appendix L: Cleaning Up Body Fluids gloves are used. Latex allergy in children: Modalities and in both the individual wearing the latex glove and the indi prevention. Guideline for disinfection and Each term has a specifc purpose and there are many sterilization in healthcare facilities. Creating a safe school for latex-sensitive Sanitize To reduce germs on inanimate surfaces to levels considered children. Disinfect To destroy or inactivate most germs on any inanimate object, but not bacterial spores. In addition, some manufacturers of cleaning products have developed ?green cleaning products. Frequent cleaning; and environmentally-friendly cleaning products appear in the b. When necessary, an application of a sanitizer or market, check to see if they are 3rd party certifed by Green disinfectant. Using a sani Appendix K: Routine Schedule for Cleaning, Sanitizing, tizer or disinfectant as this ?frst step is not efective because and Disinfecting the purpose of the solution is to either sanitize or disinfect. Having enough toys to or cots are taken out of storage during nap time, and then rotate through cleaning makes this method of preferred placed back in storage. In fact, cigarettes used by adults are the Center, Large Family Child Care Home leading cause of ignition of fatal house fres (9). Excerpts from the health consequences of good health, show no evidence of carrying any disease, involuntary exposure to tobacco smoke: A report of the Surgeon General. Department of Health and Human Services, Centers for on an intestinal parasite control program. The Health Consequences Only animals that do not pose a health or safety risk will be of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Department of Health and Human Services, Centers for Disease Control and Prevention, vised by a caregiver/teacher who is close enough to remove Coordinating Center for Health Promotion, National Center for Chronic the child immediately if the animal shows signs of distress Disease Prevention and Health Promotion, Ofce on Smoking and Health. Facts: Preventing residential The animals should be housed within some ?barrier that fre injuries.
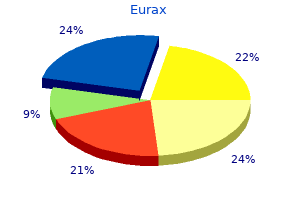
Sometimes an electrocardiogram (a painless test measuring the electrical activity of the heart) is performed to rule out heart problems acne 1 year postpartum effective eurax 20 gm. Since the cause of costochondritis is frequently unknown acne coat 20 gm eurax sale, treatment is aimed at pain control skin care quiz buy eurax master card. You may need to change your exercise routine or make adjustments to your work duties acne zones meaning purchase discount eurax line. Do not apply ice or heat for more than 15-20 minutes at a time skin care 1 month before wedding purchase 20 gm eurax mastercard, as prolonged use can increase inflammation acne 1st trimester purchase genuine eurax on-line. Consult your medical provider first if you have a history of stomach ulcers, kidney disease, or liver disease. Examples include diclofenac (Voltaren) pill or gel, amitryptyline (Elavil), and others. In severe cases unresponsive to conservative management, injection of a steroid medication into the cartilage by a specialist may be considered. Objectives To examine prevalence of signs and symptoms relative to demographics, care setting, and functional class. Methods A convenience sample of 276 patients (164 ambula tory, 112 hospitalized) with systolic heart failure completed a 1-page checklist of signs and symptoms experienced in the preceding 7 days (ambulatory) or in the 7 days before hospital ization. Recognize signs and atypical symptoms heart failure (severe cough, nausea/vomiting, diarrhea or loss that may be associated with worsening of appetite, and restlessness, confusion, or fainting, all P. Dyspnea occurred in plan related to heart failure and response all functional classes (98%-100%) and both settings (92%-100%). The incidence of heart failure continues to increase, with 660 000 new cases diagnosed annually in adults aged 45 and over. For men and women at age 40, the lifetime risk of heart failure developing is currently 1 in 5. Additionally, common signs and symptoms of heart failure may be well known to health care providers who treat heart failure routinely, but atypical signs and symptoms associated with worsening status may not be recognized at presentation. Heart failure represents a substantial burden to patients and nurses recognize signs and symptoms of the health care system, with estimated direct and heart failure and understand the management of heart indirect costs in 2008 expected to approach $35 failure, interconnections between bodily changes, sen billion,1 so it is important for health care providers sations, and behaviors may become more relevant. Behavioral models that directly or indi health status that may affect decisions about the rectly link the signs and symptoms of a disease or need for hospitalization, readiness for discharge, and condition and behavior are the Common Sense frequency of monitoring. In qualitative research, patients with ness are processed on both cognitive and emotional heart failure did not recognize common but not heart levels to form a conscious level of danger and threat specific symptoms such as dyspnea and fatigue as that leads to goals for coping and coping actions. Trochelman is a nurse researcher in nursing research the primary aim of this study was to determine and innovation at the Nursing Institute, and Jianbo Li is patients perception of signs and symptoms of heart a statistician and Songhua Lin is a statistical program mer, both in Quantitative Health Sciences, at Cleveland failure before an ambulatory visit or hospitalization. The ordinary physical activities of daily format prompted institutional review board approved the study pro living. Study candidates were 276 adults: 164 sched status if they believed ordinary symptoms they uled for an ambulatory visit in the heart failure dis physical activity did not cause ease management program (a clinic led by an undue dyspnea, fatigue, palpita were experiencing, advanced practice nurse) and 112 patients being tions, or chest pain. Convenience sampling was used to patients to report all signs and those they thought collect data for 11 months. Inclusion crite simplified to enhance patients understanding; for ria were treatment for systolic heart failure, defined example, exercise intolerance was worded as an ejection fraction of 35% or less shown by ?decreased ability to exercise or carry out activities echocardiography, age 18 years or older, alert and and paroxysmal nocturnal dyspnea was worded willing to participate, lived at home and cared for ?wake up from a sound sleep and unable to self, and understands written and spoken English. Many references described studies of individual signs and symptoms, most often fatigue, breathless time during the hospital episode. Therefore, the Ambulatory patients were asked to principal investigator developed a checklist tool of 24 check off all symptoms they had and dizziness/ signs and symptoms of heart failure, 1 question with experienced in the preceding 7 days, lightheadedness. Not sur prisingly, patients reported symptoms of heart fail Results ure much more often than they reported signs of Characteristics of Patients heart failure (Table 2). Of 24 items, the top 5 Two hundred seventy-six patients with systolic reported symptoms were shortness of breath, heart failure were included in the study. Patients char decreased ability to exercise, orthopnea, profound acteristics are provided in Table 1. Older patients were less likely to report feel Paroxysmal nocturnal dyspnea 65 (23. In appetite; right-sided abdominal pain; irregular pulse; all, 17 of 23 signs and symptoms increased signifi and palpitations (Table 3). Nearly all patients reported dyspnea skin, and low or high heart rate were rarely reported regardless of functional class. Of the paroxysmal nocturnal dyspnea remained significant signs and symptoms of heart fail functional class. For patients with higher functional class: any edema; signs and symptoms that differed by care setting, sudden weight gain; ankle edema; chest pain; severe frequencies were consistently higher in hospitalized cough; nausea/vomiting, diarrhea, or loss of patients. Although and wheezing), except that shortness these results may not seem surprising, some results In the hospital of breath and ankle and abdominal require further discussion. First, dyspnea was universally reported, regard setting, functional less of functional class or care setting. Our findings may be more comprehensive as presumably asymptomatic patients has implications a result of our use of the checklist format. Ultimately, asking about dyspnea may have recognized signs and bothersome symptoms during assessment may yield little value. Dyspnea on the checklist that they may not have thought to may be a poor marker of change in heart failure verbalize because they did not believe them to be condition unless the assessment includes other sub associated with their heart or with heart failure. Patients may not recognize dyspnea as some though the frequency of orthopnea increased signifi thing that changed if it occurred regularly or contin cantly as functional class worsened, and the preva uously. Assessment questions Patients may qualifiers should be added when questioning patients; related to new onset of paroxysmal for example, one could ask: Compared with yester nocturnal dyspnea and new onset of describe dyspnea day, do you have more shortness of breath when restlessness, confusion, or fainting on the basis of their you perform everyday activities? For example, in this lessness, confusion, or fainting increased by 101%, study, the frequency of orthopnea doubled (100% from 22. However, orthopnea was a less sensitive blood pressure, and sudden weight gain as signs marker when prevalence was compared in patients they experienced, even though the prevalence of In our study, signs that patients had a decreased appetite and food intake were reported significantly more often in hospitalized due to edema, so volume overload was offset by patients were signs reflecting fluid overload (eg, sud decreased caloric intake, or (c) volume overload was den weight gain) or hypoperfusion (change in urine offset by cachexia and loss of muscle mass. Only providers when assessing and compil a few studies have been done on fatigue in patients ysmal nocturnal ing all evidence and when developing with heart failure. Researchers29 found that in ambu dyspnea and new a diagnosis or treatment plan, but latory older women with heart failure, fatigue was such signs should be assessed as a the most frequently experienced symptom, and onset of restless group and used together to provide although it was only mildly bothersome, the fatigue support for worsening heart failure. Further, at the second assessment, fainting might be both consistent and inconsistent fatigue was associated with dyspnea. Our results may have differed signs and symptoms before admission for acute because we used the adjective profound to describe heart failure, increased abdominal girth was reported fatigue instead of ?exertional or general fatigue. Many factors study, fewer patients reported having any edema could potentially explain these findings. Patient sitive to bodily changes than are women or men related factors include heterogeneity in characteris may be quicker to communicate changes in signs tics, medical history, use and dosing of diuretics and and symptoms as heart failure worsens. Additionally, in a report of consecutive patients treated in a special patients knowledge and self-efficacy about assessing care unit for acute decompensated heart failure at edema and recognizing subtle changes could affect our site from January 2000 through December 2006,34 reporting frequency. Research is needed to determine if prevented determining the frequency of individual the cause of heart failure plays a role in the number symptoms in the cluster. Our findings reflected signs of signs and symptoms that patients report or if and symptoms that occurred at any time during a another rationale emerges. Future research with older patients is Finally, our tool did not assess needed to learn if signs and symptoms are blunted intensity, or, when applicable, loca hospitalized more with older age and if findings from this study are tion, duration, or precipitating fac similar in older patients with heart failure who have tors of signs and symptoms of heart often than women medical conditions with signs and/or symptoms that failure. Results may not be applicable research should examine relationships between signs to community-dwelling and hospitalized adults in and symptoms of heart failure and outcomes, includ other geographic regions, patients of ethnicity other ing the effects of increasing somatic awareness through than white or African American, very elderly patients, education about the signs and symptoms of heart or patients with causes of heart failure different than failure and what to do to control worsening signs the causes among our patients. It is up to health care providers to ask the right Our data collection tool was not exhaustive. When patients and failed to report them in the space provided; for use a checklist to report signs and symptoms of heart example, our tool did not include difficulty sleeping failure, both common and more atypical signs and as a symptom of heart failure. In 1 study,29 difficulty symptoms emerge, some that can be used in isola sleeping was only mildly bothersome and its inten tion and others that can be used as part of a group sity remained stable at 18 months when patients of signs and symptoms to determine current heart were resurveyed. We collected data on paroxysmal failure status and readiness for dis nocturnal dyspnea and restlessness, and, although charge, if hospitalized. Dyspnea this tool did not related, those factors are not equivalent surrogates was found in most ambulatory and of difficulty sleeping. Besides difficulty sleeping, our hospitalized patients and in include psychologi tool did not include signs or symptoms associated patients classifying themselves as with aging, such as nocturnal polyuria, even though having no limitations in activity cal signs or this also may be associated with heart failure. More (functional class I); therefore, symptoms such as over, our tool did not include signs or symptoms health care providers should not associated with depression, such as worrying or feel use the symptom dyspnea in isola those associated ing nervous, sad, or irritable, even though these tion to monitor for improvement with depression. Future research should examine signs dyspnea appears to be insensitive to heart failure or symptoms of heart failure that are associated status. A checklist may overcome patients reluc with both heart failure and depression to determine tance to report signs and symptoms believed to their independent effects on heart failure. Weight Now that you?ve read the article, create or contribute to an and symptom diary for self-monitoring in heart failure online discussion on this topic. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. A report from the American Temporal trends in clinical characteristics, treatments, and Heart Association statistics committee and stroke statistics outcomes for heart failure hospitalizations, 2002 to 2004: subcommittee. The common sense model: an organized frame six months of life in patients with end-stage heart failure. Emergency diagnosis of congestive heart failure: impact Predicting health-promoting lifestyles in the workplace. Fatigue in chronic heart failure: does effect of video education on heart failure healthcare utiliza gender make a difference? Symptoms of fatigue in chronic heart failure symptoms, and actions before a hospital admission. Range and severity of symptoms over time among older adults with chronic pulmonary disease and To purchase electronic or print reprints, contactThe heart failure. Prevalence of symptoms Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, in a community-based sample of heart failure patients. Recognize signs and atypical symptoms that may be associated with worsening heart failure and functional class. Define key elements of a patient teaching plan related to heart failure and response to treatment. Which of the following heart failure signs was 1 of the 5 most frequently heart failure for men and women at age 40? Vertigo and memory loss functional class and also was a reliable indicator of being hospitalized? Ignoring signs and symptoms as an initial coping mechanism limitation of the study data collection tool? To test the accuracy of a preprinted checklist in describing of signs and symptoms 11. To determine patients perception of signs and symptoms of heart failure with heart failure? Patients are likely to inaccurately describe the signs and symptoms of heart failure. Have these highlights do not include all the information needed to use personnel and resuscitative equipment immediately available (5. Approval: 2008 heart disease, pericarditis or pericardial effusions, stenotic carotid artery disease with cerebrovascular insufficiency, or hypovolemia (5. Some seizures are administered as an intravenous injection within 10 seconds; followed prolonged and require urgent anticonvulsive management. Adhere to the recommended duration of injection [see Dosage and Administration (2)]. As noted in an animal study, longer injection times may increase the duration and magnitude of increase in coronary blood flow [see Clinical Pharmacology (12. In clinical trials, hypersensitivity reactions were reported in fewer than 1 percent of patients [see Adverse Reactions (6. The risk of serious hypotension may be higher in patients with autonomic dysfunction, hypovolemia, left main coronary artery stenosis, stenotic valvular heart disease, pericarditis or pericardial effusions, or stenotic carotid artery disease with cerebrovascular insufficiency. In post-marketing experience, syncope, transient ischemic attacks and seizures have been observed [see Adverse Reactions (6. Most increases resolved within 10 to 15 minutes, but in some cases, increases were observed at 45 minutes following administration [see Clinical Pharmacology (12. The population was 26?93 years of age (median 66 years), 70% male and primarily Caucasian (76% Caucasian, 7% African American, 9% Hispanic, 5% Asian). Most adverse reactions began soon after dosing, and generally resolved within approximately 15 minutes, except for headache which resolved in most patients within 30 minutes. Most respiratory adverse reactions resolved without therapy; a few patients received aminophylline or a short-acting bronchodilator. Pre-specified respiratory adverse reactions included dyspnea, wheezing, obstructive airway disorder, dyspnea exertional, and tachypnea. The most common adverse reactions are similar in type and incidence to those in Table 1 above for both Groups. Table 4 shows a comparison of cardiac events of interest for the two groups [see Warnings and Precautions (5. Some events required intervention with fluids and/or aminophylline [see Overdosage (10)]. Central Nervous System Tremor, seizure, transient ischemic attack, and cerebrovascular accident including intracranial hemorrhage [see Warnings and Precautions (5. Hypersensitivity Anaphylaxis, angioedema, cardiac or respiratory arrest, respiratory distress, decreased oxygen saturation, hypotension, throat tightness, urticaria, rashes have occurred and have required treatment including resuscitation [see Warnings and Precautions (5. In animal reproduction studies, adverse developmental outcomes were observed with the administration of regadenoson to pregnant rats and rabbits during organogenesis only at doses that produced maternal toxicity (see Data). Aminophylline to Reverse Effects Methylxanthines, such as caffeine, aminophylline, and theophylline, are competitive adenosine receptor antagonists and aminophylline has been used to terminate persistent pharmacodynamic effects.
Order genuine eurax line. My Skincare Routine.