Grant E. Lattin Jr., MD
- Assistant Professor of Radiology
- Uniformed Services University of the Health Sciences
- Bethesda, Maryland
Some “first wave” cells differentiate into interstitial cells impotence jelly order discount levitra online, but cells contributing to the interstitium mostly derive from the “second wave” of cells which does not contribute to the Sertoli cell population (DeFalco et al erectile dysfunction treatment in kenya cheap levitra 20mg without a prescription. The end fate of these “second wave” cells remained uncertain until a suitable early interstitial marker could be identified erectile dysfunction question order levitra toronto. Some of the “second wave” of proliferating cells that arise after 18 ts are Mafb positive interstitial cells (DeFalco et al erectile dysfunction over the counter drugs buy levitra 20 mg with mastercard. Studies in mice and humans show that Nr5a1 mutant phenotypes are sensitive to dosage and genetic background (Luo et al erectile dysfunction doctors in louisville ky cheap levitra uk. Nr5a1-/ mice initiate early gonadal and adrenal development erectile dysfunction drugs generic buy cheap levitra 20mg, but the organs begin to regress by 11. In Nr5a1-haploinsufficient mice, adrenal and testis development was disrupted, but hypoplastic testes did form (Bland et al. These data indicate that mouse adrenal development requires both copies of Nra51 to be active, whereas the gonad can partially develop if a single copy is present. The requirement for a threshold level of Nr5a1 expression in the adrenal region and gonad is supported by phenotype of the Cited-2-/ mouse where the adrenal cortical primordium is seriously disrupted but abnormal testis differentiation can proceed. In Cited2-/ embryos, Nr5a1 levels are approximately one third of wild-type levels. As a result, the Cited2-/ embryo is often used as a proxy for attenuated Nr5a1 expression and function. As Wt1 (Wilms tumor 1) is involved in Nr5a1 regulation 16 (Wilhelm and Englert, 2002) it was expected that Cited2+/-/Wt1+/ embryos would show defects in adrenal and gonadal development. Initial reports showed that the adrenal gland of Cited2+/ /Wt1+/ embryos was small and mis-localised (Val et al. Introduction of a weakened Sry by using a Y strain was required to induce full sex reversal (Buaas et al. These findings further indicated that achieving a threshold level of Nr5a1 is essential for obtaining normal testis morphology and adrenal development in mouse. The expression of Nr5a1 is regulated by a number of tissue-specific enhancers that have been identified using reporter mouse lines. Subsequently identification of tissue-specific enhancers using transgenic mice was performed using the reductionist approach of testing regions of the proximal upstream region in transgenic reporter mice. An Sf1-LacZ reporter mouse was generated using a 674 bp fragment of the promoter that included the 500 bp region (Wilhelm and Englert, 2002). In addition, a ventromedial hypothalamus enhancer was identified in intron 6, a pituitary gonadotrope enhancer also in intron 6 and a fetal adrenal enhancer was identified in intron 4 ((Shima et al. The signaling centre of the Hh pathway, the primary cilium, is observed predominately on the interstitial cells of the fetal testis (Wainwright et al. Unfortunately, the presence of a cilium does not necessarily indicate that these populations are undergoing active Hh signaling (Rohatgi et al. Nonetheless, the expression of components of the Hh signalling pathway, such as the receptor Ptch1 (patched homolog-1; (Yao et al. In the complementary experiment, ectopic activation of the Hedgehog signalling pathway was achieved by constitutive expression of Smo using the Sf1-Cre line (“Hh-activated line”), which is active in cells throughout the ovary (Bingham et al. Ectopic activation of the pathway was sufficient to induce the differentiation of steroidogenic cells within an ovarian environment (Barsoum et al. However, it must be kept in mind that as Pdgfrα-/ testes also have defects in proliferation of Sertoli cells and mesonephric cell migration (Brennan et al. Affected males have hypothalamic dysfunction and ambiguous genitalia characterised by small testes and penis (Bonneau et al. Expression of the genes encoding markers of the steroidogenic pathway, such as Cyp11a1 and Star, are decreased from 12. Tcf21 is a basic helix-loop-helix transcription factor with multiple roles in embryonic development (Quaggin et al. Embryonically Tcf21 is expressed throughout the testis interstitium, particularly around the coelomic epithelium from 10. Hes1 expression is restricted to the interstitium, while Hes5 is expressed in the Sertoli cells at 13. Notably, germ cells and cord structure is adversely affected even though Hes1 is not expressed in these populations (Tang et al. The role of the gonads as endocrine organs also requires a functional vasculature network to facilitate the delivery and circulation of hormones to the rest of the embryo. In the process of gonadogenesis, the formation of the vasculature is important for the overall architecture and development of the testis. On the other hand, lymphangiogenesis, the formation of the lymphatic network, occurs much later in gonadal development after the architecture of the testis is mostly established. Testis vasculature is formed by migration of endothelial cells into the developing testes (Combes et al. Unlike the ovary, in the testis the early vasculature network develops by a non-angiogenic process whereby the endothelial cells migrating from the mesonephric vascular plexus are rearranged into the new network (Brennan et al. Vascularisation of the testis has been shown to play an important instructive role in testis cord formation (Combes et al. However, the mechanisms governing testis vascularisation and cord segregation are still unclear. Likewise the mechanisms governing the invasion of the venous vasculature network into the testis are not well studied. Some evidence suggests that the venous vasculature network also is derived from the mesonephros, perhaps following the establishment of the arterial vascular network (Brennan et al. Alongside the blood vascular network exists the lymphatic vascular network, which acts to maintain tissue fluid homeostasis. Using a Prox1-LacZ reporter lymphatic vessels have been detected along the gonad–mesonephric border from 13. The invading vessels originated from the pre-existing lymphatic network residing along the mesonephric region (Svingen et al. Notably the lymphatic vessels did not penetrate deep into the testis: vessels only penetrated immediately inferior to the tunica albuginea (Svingen et al. This observation 30 was consistent with previous data describing the invasion of the lymphatic vasculature network into murine testes (Hirai et al. Postnatally, interstitially residing testicular macrophages form close associations with Leydig cells (Christensen and Gillim, 1969; Hutson, 1990; Miller et al. Recently the role of macrophages in fetal testicular development has been explored. Macrophages later clustered along the expanded vascular plexus, around the coelomic vessel and alongside the vascular branches invading and enwrapping the testis. In the fetal testis a regular and ordered series of testis cords are formed by 13. In macrophage-depleted testis (approximately 95% depletion), while basic partitioning of the cord elements from the interstitial space occurred, the cords that formed were irregular (DeFalco et al. Together these data indicate that the combined invasion of endothelial cells with associated macrophages is important for testicular vascularisation, cord formation and partitioning of the testis. During postnatal life the ovary regionalises and follicular granulosa cells surround the matured germ cells, the oocytes. However, the regionalisation of the fetal ovary and the specification of the different cell lineages are poorly understood. There is a suite of genes that are important for ovarian development including Wnt4 (Vainio et al. Recently it has been demonstrated that the ovary can be regionally classified by expression of granulosa cell marker genes showing that the population of somatic cells at or adjacent to the coelomic epithelium are distinct from the cells adjacent to the mesonephros (Chen et al. Based on gene expression, another study has classified the somatic cell lineages of the ovary into four somatic lineages: vasculature; vascular associated; somatic coelomic epithelial and pre-granulosa cell populations ((Maatouk et al. It is clear that there are two classes of pre-granulosa cells in the fetal mouse ovary (Mork et al. These follicles are 32 important for the onset of puberty and early fertility (Zheng et al. The cortical follicles progressively mature and constitute the reproductive pool of primordial follicles for the individual throughout their reproductive life (for review see Monget et al. The theca cells first produce steroids after birth in the preantral follicle (Palermo, 2007). No markers of the embryonic theca progenitor cell population have yet been identified. Identifying additional cell-lineage specific markers will provide new tools investigate the development and maturation of the ovary. A series of somatic subpopulations have been defined using different marker genes. Several genes have been identified as key players in ovarian development but no ovarian-determining factor has yet been identified. Additionally, in the Rspo1-/ ovary, the male Wolffian duct fails to regress, ectopic steroidogenic cells differentiate and a masculinised vasculature forms, features reminiscent of the Wnt4-/ ovary (Tomizuka et al. The effect of removing functional β-catenin in the somatic ovarian cells was a downregulation of the expression of the genes encoding Wnt4 and Fst, but not Rspo1 (Liu et al. These data implicate β-catenin in the process of vascular remodeling and germ cell survival in all these scenarios. Using a tamoxifen-inducible Cre/loxP system it has been demonstrated by Uhlenhaut et al. The sexual fate of the germ cell is determined by signalling factors that the germ cells are exposed to upon entry to the gonad, rather than by their chromosomal constitution (Adams and McLaren, 2002; Bowles et al. Much of what is known about the origin and regulation of germ cell identity is derived from studies in mice, as discussed below. As germ cells are not the focus of the work presented in this thesis the following provides only a brief overview of germ cell development. In an ovary, germ cells must enter meiosis during fetal life if they are to initiate oogenesis correctly; conversely, meiosis must be avoided in male germ cells in the fetus if they are to embark on the spermatogenic pathway. Regardless, a strong antagonism exists between meiosis-promoting (female) factors and meiosis-suppressing (male) factors that push the resident germ cells into their respective fates. Stra8-/ mice are infertile, with meiosis defects evident in the fetal ovary (Baltus et al. A comprehensive understanding of the mechanisms surrounding germ cell entry into meiosis in the fetal ovary and postnatal testis will be important as incorrect meiotic progression can result in infertility and germ cell tumours. One of the primary challenges facing the community is the functional validation of all the candidate genes being identified. As a result there have been numerous attempts to develop a methodology to assess gene function during development of embryos and organs to enable pre-screening candidate genes. In the field of gonadal development knockdown protocols have been based on modification of established ex vivo organ culture methods. The two major considerations have been the type of construct delivered and the construct delivery method. Delivery methods have included injection, electroporation or liposome-based introduction of the construct into the tissue. This approach achieved a variable rate of delivery, the construct was expressed in approximately 20% of cells, but these cells were mainly localised around the injection site (Svingen et al. A major concern with these methodologies was that the delivery of the construct was predominately restricted to near the injection site where the damage to the tissue by the blunt force of the injection made interpreting phenotype difficult. An immediate decrease in protein may not be observed, as pre existing protein must be degraded before protein signal decreases. However, it is possible that an abnormal protein retaining some activity will be produced. Using this approach branching morphogenesis defects were detected in targeted explants (Dean et al. Subsequent work in the kidney used media supplemented with 10 µM vivo-morpholino, but others have failed to reliably replicate this work ((Hartwig et al. Therefore, ex vivo knockdown of gene function in organ culture remains a key challenge for the field in functionally validating the roles of genes of interest. The critical importance of endocrine function in reproduction and general health has meant that Leydig cells, in the postnatal and adult context, have been studied extensively. This volume of genes needing functional validation will require more efficient screening methods to be developed. In this work, we knocked down Stra8, Sox9, Gli1/2, Ctrb1 and Adamts19 in the fetal gonad and Sox9 in the fetal pancreas. In addition we targeted two genes with roles in early gonadogenesis, Wnt4 and Nr0b1, and Gli3, a hedgehog pathway member. Furthermore, I used this technique to investigate the role of putative disease causing genes during gonad development. This work was part of an ongoing collaboration with Stefanie Eggers and Andrew Sinclair (Murdoch Childrens Research Institute, Australia). On top of these data, whole exome and whole genome sequencing of rare disease cohorts has identified a plethora of possible causative genes for human developmental disorders, and these too require validation. Modelling genetic mutations in human development, physiology and disease in the mouse model has provided invaluable insights. Considering that there is a significant risk that a knockout of a gene may result in embryonic lethality or little to no phenotype, the generation of a loss-of-function mouse model for every interesting candidate remains impractical. In order to prioritise candidates for further characterisation we need to develop a technique to assess the probable effects that the loss-of function of a gene-of-interest may have on organogenesis. To address this need I developed a method to knock down gene function in the mid-gestation mouse embryo, and then culture the organs ex vivo. There were two main hurdles to overcome in developing this strategy for mouse tissues: delivery of the compound and the nature of the compound itself.
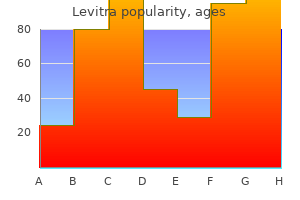
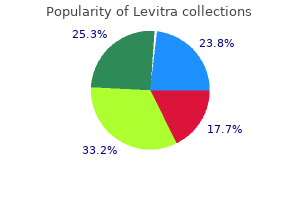
The phenotypic variability of genetic traits can be studied in monozygous twins shakeology erectile dysfunction buy discount levitra online, and the effect of a shared intrauterine environment may be studied in Dichorionic diamniotic Monochorionic monoamniotic dizygous twins erectile dysfunction 21 years old purchase discount levitra on line. Examination of the placenta and membranes may help to distinguish between monozygous and dizygous twins but is not completely reliable erectile dysfunction treatment electrical purchase levitra 10 mg without prescription. Only rarely is diabetes caused by the secretion dependent dependent diabetes diabetes of an abnormal insulin molecule what causes erectile dysfunction levitra 10 mg low cost. Genetic Ketosis No ketosis predisposition is important impotence vitamins order generic levitra on-line, but only 30% of monozygous Early onset Late onset twins are concordant for the disease and this indicates that Treatment Insulin Diet or drugs Concordance in monozygotic twins 30% 40–100% environmental factors (such as triggering viral infections) Histocompatibility antigens Associated Not associated are also involved erectile dysfunction treatment mumbai trusted 10mg levitra. The Antibodies to insulin and islet cells Present Absent overall risk to siblings is about 6%. Monozygous twin 30 High risk haplotypes have a different amino acid at this Non-insulin dependent diabetes position and homozygosity for non-aspartic acid residues is First degree relative 10–40 found much more often in diabetics than in non-diabetics. Susceptibility is First degree relative 50 dependent on the length of a 14bp minisatellite repeat unit. There is a strong genetic predisposition although other factors such as obesity are important. Concordance in monozygotic twins is 40–100% and the risk to siblings may approach 40% by the age of 80. High circulating Lp(a) lipoprotein concentration has been suggested to have a population attributable risk of 28% for myocardial infarction in men aged under 60. The risk of coronary heart disease increases with age in heterozygous subjects, who may also have xanthomas. Familial aggregations of early coronary heart disease also occur in people without any detectable abnormality in lipid metabolism. Risks to other relatives will be high, and known environmental triggers should be avoided. Future molecular genetic studies may lead to more precise identification of subjects at high risk as potential candidate genes are identified. Schizophrenia and affective psychoses A strong familial tendency is found in both schizophrenia and affective disorders. The importance of genetic rather than environmental factors has been shown by reports of a high incidence of schizophrenia in children of affected parents and Figure 12. The recurrence (%) in schizophrenia and affective psychosis same is true of manic depression. Empirical values for lifetime according to affected relative risk of recurrence are available for counselling, and the burden of the disorders needs to be taken into account. Both polygenic Affective and single major gene models have been proposed to explain Schizophrenia psychosis genetic susceptibility. A search for linked biochemical or Incidence in general molecular markers in large families with many affected population 1 2–3 members has so far failed to identify any major susceptibility Sibling 9 13 genes. Some malformations are non-genetic, such as the amputations caused by amniotic bands after early rupture of the amnion. Decisions to have further Congenital heart disease 1–4 children will be influenced by the fact that the risk of Cleft lip and palate 4 recurrence is generally low and that surgery for many isolated Cleft palate alone 2 congenital malformations is successful. Prenatal Renal agenesis 3 ultrasonography may identify abnormalities requiring Pyloric stenosis 2–10† Congenital dislocated hip 1–11† emergency neonatal surgery or severe malformations that have a poor prognosis, but it usually gives reassurance about the Club foot 3 Hypospadias 10 normality of a subsequent pregnancy. Cryptorchidism 10 Tracheo-oesophageal fistula 1 Exomphalos 1 *Risk reduced by periconceptional supplementation with folic acid † Risk affected by sex of index case or sibling, or both Mental retardation or learning disability Intelligence is a polygenic trait. Mild learning disability (intelligence quotient 50–70) represents the lower end of the normal distribution of intelligence and has a prevalence of about 3%. The intelligence quotient of offspring is likely to lie around the mid-parental mean. Intelligent parents who have one Risk child with mild learning disability are less likely to have another similarly affected child. One sibling 1 in 35 By contrast, the parents of a child with moderate or severe male sibling 1 in 25 learning disability (intelligence quotient 50) are usually female sibling 1 in 50 One sibling (consanguineous of normal intelligence. A specific cause is more likely when parents) 1 in 7 the retardation is severe and may include chromosomal Two siblings 1 in 4 abnormalities and genetic disorders. The risk of recurrence Male sibling plus maternal uncle depends on the diagnosis but in severe non-specific retardation or male cousin X linked is about 3% for siblings. A higher recurrence risk is observed after the birth of an affected male because some of these cases represent X linked disorders. Recurrence risks are also higher (about 15%) if the parents are consanguineous, because of the increased likelihood of an autosomal recessive aetiology. The recurrence risk for any couple increases to 25% after the birth of two affected children. This chromosomal abnormality may not and aetiology of structural developmental defects. Animal be detected by routine cytogenetic research is providing information about cellular interactions, analysis. Recognition of clinical migration and differentiation processes, and gives insight into features and fluorescence in situ hybridisation analysis enables the possible mechanisms underlying human malformations. Diagnosing multiple congenital abnormality syndromes in children can be difficult but it is important to give correct advice about management, prognosis and risk of recurrence. Definition of terms Malformation A malformation is a primary structural defect occurring during the development of an organ or tissue. An isolated malformation, such abdominal organs through the as cleft lip and palate, congenital heart disease or pyloric abdominal wall defect. Most single may occur as an isolated anomaly or malformations are inherited as polygenic traits with a fairly low as part of a multiple malformation syndrome or chromosomal disorder risk of recurrence, and corrective surgery is often successful. Multiple malformation syndromes comprise defects in two or more systems and many are associated with mental retardation. The risk of recurrence is determined by the aetiology, which may be chromosomal, teratogenic, due to a single gene, or unknown. Minor anomalies are those that cause no significant physical or functional effect and can be regarded as normal variants if they affect more than 4% of the population. The presence of two or more minor anomalies indicates an increased likelihood of a major anomaly being present. Disruption A disruption defect implies that there is destruction of a part of a fetus that had initially developed normally. Disruptions usually affect several different tissues within a defined anatomical region. Amniotic band disruption after early rupture of the amnion is a well-recognised entity, causing constriction bands that can lead to amputations of digits and Figure 13. Sometimes more extensive disruptions occur, such as constriction bands as a consequence of amniotic band disruption facial clefts and central nervous system defects. Interruption of the blood supply to a developing part from other causes will also cause disruption due to infarction with consequent atresia. As the fetus is genetically normal and the defects are caused by an extrinsic abnormality the risk of recurrence is small. Deformation Deformations are due to abnormal intrauterine moulding and give rise to deformity of structurally normal parts. Deformations usually involve the musculoskeletal system and may occur in fetuses with underlying congenital neuromuscular problems such as spinal muscular atrophy and congenital myotonic dystrophy. In these disorders arthrogryposis due to amyoplasia 68 Dysmorphology and teratogenesis the prognosis is often poor and the risk of recurrence for the underlying disorder may be high. Oligohydramnios causes fetal deformation and is well recognised in fetal renal agenesis (Potter sequence). The absence of urine production by the fetus results in severe oligohydramnios, which in turn causes fetal deformation and pulmonary hypoplasia. A normal fetus may be constrained by uterine abnormalities, breech presentation or multiple pregnancy. The prognosis is generally excellent, and the risk of recurrence is low except in cases of structural uterine abnormality. Dysplasia Dysplasia refers to abnormal cellular organisation or function within a specific organ or tissue type. Unlike the other mechanisms causing birth Service, St Mary’s Hospital, Manchester) defects, dysplasias may have a progressive effect and can lead to continued deterioration of function. Classification of birth defects Single system defects Single system defects constitute the largest group of birth defects, affecting a single organ system or local region of the body. The commonest of these include cleft lip and palate, club foot, pyloric stenosis, congenital dislocation of the hip and congenital heart defects. Each of these defects can also occur frequently as a component of a more generalised multiple abnormality disorder. Congenital heart defects, for example, are associated with many chromosomal disorders and malformation syndromes. When these defects occur as isolated abnormalities, the recurrence risk is usually low. Identification of a birth defect syndrome allows comparison of cases to define the clinical spectrum of the disorder and aids research into aetiology and pathogenesis. Sequences the term sequence implies that a series of events occurs after a single initiating abnormality, which may be a malformation, a deformation or a disruption. The features of Potter sequence are classed as a malformation sequence because the initial abnormality is renal agenesis, which gives rise to oligohydramnios and secondary deformation and pulmonary Figure 13. Other examples are the holoprosencephaly occuring as part of Apert syndrome in a child with craniosynostosis due sequence and the sirenomelia sequence. In holoprosencephaly to a new mutation in the fibroblast growth factor receptor-2 gene the primary developmental defect is in the forebrain, leading to microcephaly, absent olfactory and optic nerves, and midline defects in facial development, including hypotelorism or cyclopia, midline cleft lip and abnormal development of the nose. In sirenomelia the primary defect affects the caudal axis of the fetus, from which the lower limbs, bladder, genitalia, kidneys, hindgut and sacrum develop. The names given to recognised malformation associations are often acronyms of the component abnormalities. Hence the Vater association consists of vertebral anomalies, anal atresia, tracheo-oesophageal fistula and radial defects. The acronym vacterl has been suggested to encompass the additional cardiac, renal and limb defects of this association. Murcs association is the name given to the non-random occurrence of Mullerian duct aplasia, renal aplasia and cervicothoracic somite dysplasia. In the Charge association the related abnormalities include colobomas of the eye, heart defects, choanal atresia, mental retardation, growth retardation and ear anomalies. The underlying aetiology may represent a vascular event, resulting in the defects such as those seen in hemifacial microsomia (Goldenhar syndrome), Poland anomaly and some cases of Möbius syndrome. Parents often experience feelings of guilt after the birth of an abnormal child, and time spent discussing what is known about the aetiology of the abnormalities may help to alleviate some of their fears. They also need an explanation of what to expect in terms of treatment, anticipated complications and long term outlook. Accurate assessment of the risk of recurrence cannot be made without a diagnosis, and the availability of prenatal diagnosis in subsequent pregnancies will depend on whether Figure 13. Parental age and family history may provide clues fluorescence in situ hybridisation analysis about the aetiology. Any abnormalities during the pregnancy, including possible exposure to teratogens, should be recorded, as well as the mode of delivery and the occurrence of any perinatal problems. The subsequent general health, growth, developmental progress and behaviour of the child must also be assessed. Examination of the child should include a search for both major and minor anomalies with documentation of the abnormalities present and accurate clinical measurements and photographic records whenever possible. Investigations required may include chromosomal analysis and molecular, biochemical or radiological studies. A chromosomal or mendelian aetiology has been identified for many multiple congenital malformation syndromes enabling appropriate recurrence risks to be given. Consanguineous marriages may give rise to autosomal recessive syndromes unique to a particular family. In this situation, the recurrence risk for an undiagnosed multiple malformation syndrome is likely to be high. In any family with more than one child affected, it is appropriate to explain the 1 in 4 risk of recurrence associated with autosomal recessive inheritance, although some cases may be due to a cryptic familial chromosomal rearrangement. The molecular basis of an increasing number of birth defect syndromes is being defined, as genes involved in various processes instrumental in programming early embryonic development are identified. Numerous malformation syndromes have been identified, and many are extremely rare. Published case reports and specialised texts often have to be reviewed before a diagnosis can be reached. Computer programs are available to assist in differential diagnosis, but despite this, malformation syndromes in a considerable proportion of children remain undiagnosed. Stillbirths Detailed examination and investigation of malformed fetuses and stillbirths is essential if parents are to be accurately counselled about the cause of the problem, the risk of Figure 13. As with liveborn infants, careful documentation of Professor Dian Donnai, Regional Genetic Service, St. Mary’s Hospital the abnormalities is required with detailed photographic Manchester) records. Cardiac blood samples and skin or cord biopsy specimens should be taken for chromosomal analysis and bacteriological and virological investigations performed. Autopsy will determine the presence of associated internal abnormalities, which may permit diagnosis. Although fairly few drugs are proved teratogens in Manchester) humans, and some drugs are known to be safe, the accepted policy is to avoid all drugs if possible during pregnancy. Thalidomide has been the most dramatic teratogen identified, and an estimated 10000 babies worldwide were damaged by this drug in the early 1960s before its withdrawal.
The consumer also needs to be made aware of the impact on risk from different preparation and cooking times of shellfish erectile dysfunction causes heart disease order levitra 20mg otc, as the risks attached to eating raw erectile dysfunction doctor in kuwait buy levitra with amex, cooked and smoked oysters erectile dysfunction in young males purchase levitra 20 mg otc, raw and cooked prawns and raw erectile dysfunction at the age of 25 levitra 10 mg without a prescription, cooked and smoked mussels will all be different erectile dysfunction statistics uk levitra 20mg lowest price. Currently erectile dysfunction pills from india generic 20 mg levitra with amex, consumers generally rely on food labels for advice which most food manufacturers and retailers provide on food preparation, for example, there is now distinct advice on the cooking of oysters, mussels and cockles. The term “shellfish” could be too vague to some consumers and making this clear would be helpful. This should include advice on the need to maintain good hygiene in the home as this is the most important advice for consumers. This should include the fact that the risk of norovirus, associated with eating raw bivalves from seawater, is higher during the winter months. Summary of conclusions and recommendations For ease of reference, this Chapter summarises the conclusions we have reached throughout this report and the recommendations we have made. We have endeavoured to prioritise the recommendations by separating these into recommendations that we consider will inform risk assessments and those that will impact on risk assessments. For those recommendations that inform on risk assessments we have undertaken to identify the lead Department that should take these forward. Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R3. Page 97 of 136 Recommendations Recommendations that Inform Risk Assessments* Lead department/s R4. The impact of foodborne transmission in health and social care settings, in particular, may be higher than is currently recognised because the possibility of foodborne transmission in these settings is likely to be under-investigated. Page 98 of 136 In almost all incidents where a viral aetiology is suspected proper investigation is not performed. Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R5. The direct impact at population level is likely to be small, given that the people who eat raw bivalves are probably relatively limited in number. However, the contribution of raw bivalves to the overall burden 41 Management of outbreaks of foodborne illness in England and Wales. Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R6. Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R7. Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R8. Contamination of the environment Conclusions Our current understanding is that symptomatic infected food handlers constitute the single most common source of foodborne norovirus. Page 104 of 136 Recommendations Recommendations that Inform Risk Assessments* Lead Department/s R9. Consumer awareness Conclusions Authoritative information on risks associated with different foodstuffs and definitive cooking instructions is hard to find on Government websites. Page 105 of 136 Recommendations Recommendations that Impact on Risk Assessments* R11. For instance, there should be advice on cooking shellfish and pork products as well as information on washing leafy green vegetables and soft fruit. Antibody A protein formed in direct response to the introduction into an individual of an antigen. Antigen A substance which elicits an immune response when introduced into an individual. Asymptomatic An infection with a microorganism where the person infected infection does not suffer any resulting symptoms or disease. Avian influenza Influenza virus subgroup which can be found in birds, but can also infect humans. Bacterium A microscopic organism with a rigid cell wall – often unicellular and multiplying by splitting in two – which has the ability to live freely. Biocide Biological/chemical means of controlling or destroying a harmful organism. Bivalve molluscs Filter feeders with two shells that process large amounts of seawater to obtain their food. Page 110 of 136 Campylobacter Gram-negative bacteria with a characteristic spiral shape. Harvested animals are transferred to tanks of clean seawater where they continue to filter feed for a period during which time sewage contaminants are purged out by normal physiological processes. Electron Microscopy that uses a beam of electrons as the radiation microscopy source for viewing a specimen. Enteric virus Any virus which enters the body through the gastrointestinal tract, multiplies there, and is usually transmitted by the faecal/oral route. Enterovirus Any virus which enters the body through the gastrointestinal tract, multiplies there, and has a tendency to invade the central nervous system. Enzyme A protein which acts as a highly efficient and specific biological catalyst. Enzyme-linked An assay in which an enzyme is used (as a marker) to indicate Immunosorbent the presence of specific antigens or antibodies. Assay Epidemiology the study of factors affecting health and disease in populations and the application of this study to the control and prevention of disease. Gastroenteritis Inflammation of the stomach and the intestine, usually due to Page 111 of 136 infection by bacteria, viruses, or food poisoning toxins, causing vomiting and diarrhoea. Herd immunity the collective immunity or resistance to a given disease exhibited by a community or population (human or animal) in the setting of its own environment. Human normal A solution which contains antibodies derived from the plasma of immune globulin donated blood IgA, IgG, IgM Different types of immunoglobulin found in body fluids. Immunity the body’s ability to resist infectious disease, afforded by the presence of circulating antibodies and white blood cells. Immunoassay Any procedure in which the specificity of the antigen-antibody reaction is used for detecting or quantifying antigens, antibodies or substances. Immunoglobulins A group of structurally-related proteins which are antibodies found in body fluids. Immunotherapy Suppression, enhancement or induction an immune response to treat an illness. Used to describe biological processes made to happen in laboratory apparatus, outside a living organism. Incubation period the time interval between the initial entry of a pathogen into a host, and the appearance of the first symptoms of disease. Jaundice the yellowing of the skin, or the whites of the eyes, indicating excess bilirubin (a bile pigment) in the blood. Kaplan’s criteria Criteria (clinical and epidemiological) for norovirus outbreaks developed by Kaplan in the 1980s. Listeria Gram-positive anaerobic, pathogenic bacteria which causes the monocytogenes listeriosis infection. Monovalent A vaccine which contains one type of substance which can elicit vaccine an immune response when introduced into an individual. Multivalent A vaccine which contains several different types of substance vaccine which can elicit an immune response when introduced into an individual. Nipah virus Emerging zoonotic virus with a large genome, capable of infecting various different types of host. Oligonucleotides Short length polynucleoside chains, usually less than 30 residues long. Organoleptic Qualities of food experienced by the senses, such as taste and smell. Pasteurisation A form of heat treatment which kills vegetative pathogens and spoilage bacteria in milk and other foods. Page 113 of 136 Pasteurisation Time taken, at a given temperature, for the pasteurisation value process to take place, ensuring that the number of microbes present is reduced to a safe value. Phylogenetic Relating to the evolutionary history of a species or taxonomic group. Prophylactic Treatment, usually immunologic, designed to protect an individual from the future development of a condition or disease. It particularly affects young children and infants with the symptoms of severe diarrhoea and dehydration. Sapoviruses Viruses which belongs to the Caliciviridae family which can cause acute gastroenteritis. Sensitive waters Estuaries, bays and other coastal waters where there is poor water exchange with the ocean and which are therefore susceptible to eutrophication. Seroprevalence the persistence of serotype-specific serum antibodies, following infection with a given pathogen. Serum Essentially similar to plasma (the fluid part of the blood), but lacking fibrinogen and other substances active in the coagulation process. Severe acute Viral disease that affects the respiratory system which is respiratory caused by the severe acute respiratory syndrome coronavirus. Small round the viral agents most commonly associated with foodborne structured viruses viral infections. Species A classification or organisms within a genus which have similarities and can be further sub-divided into sub-species. Staphylococcus Small, round, non-motile bacteria that is commonly found in aureus clusters. Strain A population of organisms within a species or sub-species distinguished by sub-typing. Vaccination Administration of a biological preparation to stimulate the immune system to develop immunity against a particular pathogen. Vaccine adjuvant Agent combined with a vaccine which allows the host’s immune response to be enhanced. Viral Inflammation of the stomach and the intestine due to infection gastroenteritis by viruses. Virion An infectious particle responsible for transporting the viral genome from cell to cell. Virus A sub-microscopic organism which is only capable of replication within living cells. Virus-like particle Particles that do not contain any viral genetic material and so are not infectious, despite having a likeness to viruses. Zoonoses Vertebrate animal host infections that can be transferred to humans naturally. Trends in indigenous foodborne disease and deaths, England and Wales: 1992 to 2000. Rotavirus survival on human hands and transfer of infectious virus to animate and nonporous inanimate surfaces. Norovirus outbreak of probably waterborne transmission with high attack rate in a Guatemalan resort. Foodborne virus inactivation by thermal and non-thermal processes In: Food and Waterborne Viruses (Cook, N. Survival and transfer of murine norovirus 1, a surrogate for human noroviruses, during the production process of deep-frozen onions and spinach. Molecular characterization of G11P[25] and G3P[3] human rotavirus strains associated with asymptomatic infection in South India. Thermal inactivation of infectious hepatitis E virus in experimentally contaminated food. Prevalence and transmission of hepatitis E virus in domestic swine populations in different European countries. Contamination of foods by food handlers: experiments on hepatitis A virus transfer to food and its interruption. Molecular and epidemiologic trends of caliciviruses associated with outbreaks of acute gastroenteritis in the United States, 2000-2004. Molecular epidemiology of caliciviruses detected in sporadic and outbreak cases of gastroenteritis in France from December 1998 to February 2004. Close similarity between sequences of hepatitis E virus recovered from humans and swine, France, 2008-2009. A community outbreak of food borne small round-structured virus gastroenteritis caused by a contaminated water supply. Effects of sanitation, freezing and frozen storage on enteric viruses in berries and herbs. Gastroenteritis associated with Tomales Bay oysters: investigation, prevention and control. Trends in the levels of Escherichia coli in commercially harvested bivalve shellfish from England and Wales, 1999–2008. Viral gastroenteritis associated with eating oysters – Louisiana, December 1996–January 1997. Spatial and temporal pattern of th norovirus contamination in a Pacific oyster fishery. Proceedings of the 9 International Conference on Molluscan Shellfish Safety, 2009. Sanitary profiles of selected shellfish water catchments pre and post-improvements in sewerage infrastructure. Public health threat of new, reemerging, and neglected zoonoses in the industrialized world. Nucleic acid amplification based methods for detection of enteric viruses: definition of controls and interpretation of results. A foodborne outbreak of gastroenteritis associated with Norwalk-like viruses: first molecular traceback to deli sandwiches contaminated during preparation.
Increased echogenicity of fetal kidneys in the first trimester can be a sign of associated renal dysplasia erectile dysfunction causes agent orange discount levitra 20mg online, aneuploidy ritalin causes erectile dysfunction purchase levitra online, or cystic renal disease erectile dysfunction creams and gels buy levitra 10 mg free shipping. A and B: Hyperechogenic kidneys (arrows) in the first trimester in association with posterior urethral valves erectile dysfunction age 27 20 mg levitra amex. C and D: Hyperechogenic kidneys (arrows) in the first trimester in association with trisomy 13 erectile dysfunction drug companies 10 mg levitra for sale. Facial dysmorphism erectile dysfunction forums cheap levitra online master card, cardiac anomaly, and other abnormalities were also seen on ultrasound (not shown). Note in B, the presence of hyperechogenic kidneys, a common finding in trisomy 13. Note the presence of bilaterally enlarged polycystic kidneys, seen transabdominally in A and C and transvaginally in B. D: An axial plane of the lower pelvis in color Doppler shows the two umbilical arteries with no bladder seen in between. Amniotic fluid is still normal at this gestation and typically disappears around 16 weeks. This pregnancy was the result of consanguineous couple with recurrence risk of 25%. Note in A the presence of an occipital encephalocele and in B the presence of bilateral polycystic kidneys (arrows). B: A coronal plane of the abdomen in the next pregnancy at 12 weeks of gestation, showing normal size kidneys (one shown—arrow) with mild hyperechogenicity: within the echogenicity range of normal kidneys in early gestation (compare with Fig. Ultrasound Findings Ideally, the kidneys should be visualized in a sagittal or coronal view in order to demonstrate large segments of renal parenchyma and enable a comparison with the surrounding lung, liver, and bowel. Enlarged hyperechogenic kidneys in the first trimester are particularly concerning because of the possibility of polycystic kidney disease or the association with aneuploidies (Fig. Disease manifestation in childhood or in 24,25 adulthood is the most common presentation. Out of the ciliopathies group is Meckel–Gruber syndrome, with the triad of polycystic kidneys, encephalocele, and polydactyly (Figs. When normal or mildly hyperechogenic kidneys are noted in the first trimester in at-risk families, follow-up ultrasound examinations into the second and third trimester is important because progression of ultrasound findings tend to occur after mid-gestation. In fetuses with Meckel–Gruber syndrome, enlarged cystic kidneys are commonly seen in 21 the first trimester along with the presence of a posterior encephalocele and polydactyly (Figs. Associated Findings Differential diagnosis of enlarged echogenic kidneys in the first trimester includes normal variant, trisomy 13, trisomy 18, adult-onset polycystic kidney disease, Meckel–Gruber syndrome, and/or other ciliopathies. The presence of enlarged hyperechogenic kidneys can occasionally be seen in early gestation, typically in the presence of a family history. The presence in the first trimester of an absent bladder on repeated examinations is also possible, given the lack of renal function. Extrarenal anomalies include central nervous 26 system, cardiac, and gastrointestinal. Bilateral Renal Agenesis Definition Bilateral renal agenesis is defined by the congenital absence of both kidneys and ureters, and results from a developmental failure of the ureteric bud and/or the metanephric mesenchyme. Bilateral renal agenesis has a prevalence of 1:4,000 to 1:7,000 pregnancies at the routine obstetric ultrasound 27 examination. The absence of both kidneys results in anhydramnios, which is typically first noted after 16 weeks of gestation. Anhydramnios leads to Potter sequence, which is a constellation of findings including pulmonary hypoplasia, facial abnormalities, and deformities of extremities. Bilateral renal agenesis is more common in males and is a uniformly lethal malformation. Ultrasound Findings the prenatal diagnosis of bilateral renal agenesis is a straightforward diagnosis after 16 weeks, because of associated oligohydramnios, as a leading ultrasound clue. The onset of oligo or anhydramnios starts between 15 and 16 weeks of gestation when amniotic fluid production is primarily renal in origin. Therefore, the suspicion of bilateral renal agenesis in the first trimester is a challenge and primarily relies on the identification of an absent bladder and kidneys (Figs. Absent bladder in the pelvis on repeated ultrasound examinations may alert the examiner to 28 the presence of bilateral renal agenesis in the first trimester. Color Doppler applied on an axial view of the pelvis will identify the two umbilical arteries and help to localize the anatomic site of the bladder (Figs. On rare occasions, a small “bladder” maybe visible in the pelvis in early gestation despite the presence of bilateral renal agenesis. Although the exact etiology of this finding is currently unclear, possibilities include retrograde filling of the bladder or the 28 presence of a midline urachal cyst mimicking the bladder. A coronal plane of the abdomen and pelvis in color Doppler will identify the descending aorta and the absence of renal arteries (Figs. The “lying down” or “flat” adrenal sign, an important second trimester sign showing the flattened adrenal gland on the psoas muscle, is not easily seen in the first trimester (Fig. When bilateral renal agenesis is suspected in the first trimester, follow-up ultrasound in the early second trimester is recommended to confirm the diagnosis by the onset of anhydramnios. Associated Malformations Associated malformations have been frequently reported and include gastrointestinal, vascular, and laterality defects. Chromosomal aneuploidy 27 is present in about 7% of prenatal cases, and several causative gene mutations have been described. The absence of a bladder on ultrasound in the first trimester should also alert the examiner to the presence of other urogenital malformations such as bladder exstrophy or bilateral cystic renal 1 dysplasia. In B, renal arteries could not be imaged with empty renal fossa and absence of renal arteries bilaterally. The presence of a pelvic kidney could not be ruled out, and the patient had a follow-up ultrasound at 16 weeks of gestation (not demonstrated) showing anhydramnios and confirming the diagnosis of bilateral renal agenesis. Note the presence of the typical flat adrenal gland (labeled) in A and B and compare with the normal shape of the adrenal gland in Figure 13. Fetus in A also had a single umbilical artery, which led us to perform a transvaginal detailed ultrasound. Fetus in B had a cardiac defect, diagnosed at 12 weeks of gestation and detailed first trimester ultrasound revealed the presence of an empty renal fossa with flat adrenal gland (asterisk). Unilateral Renal Agenesis Unilateral renal agenesis results when one kidney fails to develop and is absent. This is primarily because of failure of development of the ureteric bud or failure of induction of the metanephric mesenchyme. The prenatal diagnosis in the first trimester is initially suspected when one kidney is not seen in the renal fossa (Fig. A search for a pelvic kidney or crossed ectopia should be performed before the diagnosis of unilateral renal agenesis is confirmed. Color Doppler of the abdominal aorta, obtained in a coronal plane of the abdomen and pelvis, is helpful to confirm the diagnosis because it shows the absence of a renal artery on the suspected renal agenesis side. In high resolution ultrasound, visualization of the renal fossa can reveal the presence of the horizontal flat (lying down) adrenal gland instead of the kidney (Fig. Compensatory hypertrophy of the contralateral kidney is present in the second and third trimester of pregnancy. The diagnosis of a single umbilical artery in the first trimester presents an increased risk for renal malformations. Pelvic Kidney, Crossed Renal Ectopia, and Horseshoe Kidney Abnormal kidney location, also referred to as renal ectopia, encompasses three types of abnormalities: pelvic kidney, crossed renal ectopia, and horseshoe kidney. Abnormal kidney location results from failure of proper migration of the metanephros from the pelvis to the abdomen during embryogenesis. Pelvic kidney refers to a kidney that is located in the pelvis below the aortic bifurcation (Fig. Crossed renal ectopia refers to two kidneys on one side of the abdomen, with fusion of the kidneys. Horseshoe kidney, the most common form of renal ectopia, refers to fusion of the lower poles of the kidneys in the midline abdomen, typically below the origin of the inferior mesenteric artery (Fig. In the first trimester, the slightly bright appearance of kidneys helps in the identification of kidney location in the pelvis when the renal fossa appears empty (Fig. Bridging of renal tissue over the fetal spine helps in the identification of a horseshoe kidney in the first trimester (Fig. In our experience, the presence of trisomy 18, Turner syndrome, and single umbilical artery increases the risk for an association with horseshoe kidneys (Fig. Duplex Kidney Duplex kidney, also referred to as duplicated collecting system, occurs when a kidney is divided into two separate moieties, an upper moiety and a lower moiety. Duplex kidney is thought to occur during embryogenesis when an additional ureteric bud arises from the mesonephric duct and fuses with the metanephric mesenchyme. The ureter arising from the upper renal moiety is commonly dilated and may form an ureterocele in the bladder, which is a common sign leading to its prenatal diagnosis. The renal pelvis of the upper moiety is also commonly dilated and has a “cyst-like” appearance on 29 prenatal sonography. Duplex kidney is more common in females and is present bilaterally in about 15% to 20% of cases. The suspicion of duplex kidney in the first trimester is rare, and the diagnosis is, however, feasible when alerted by family history. The presence of two renal pelves in one kidney on coronal view suggests the diagnosis. Note the presence in A of a left pelvic kidney (arrow) and a flat adrenal gland (asterisk). B: the same figure as in A, with annotations to display both kidneys and adrenals. Note the normal triangular shape of the adrenal on the right (R) side and the flat left (L) adrenal. The left pelvic kidney is shown in the pelvis as opposed to the abdominal location of the right kidney. Because of the increased echogenicity in the kidneys in the first trimester, the renal bridge between the right and left kidney across the midline can be well appreciated. Fetus in B also had cystic hygroma and body edema (double headed arrow) and the diagnosis of monosomy X was confirmed. Bladder Exstrophy and Cloacal Abnormalities Bladder exstrophy is a defect of the anterior lower abdominal wall, inferior to the insertion of the umbilical cord, and involving the protrusion of the urinary bladder. Typically, the umbilical cord inserts low on the abdominal wall, and the bladder mucosa is eventrated directly below the umbilical cord. Bladder exstrophy occurs more commonly in males than in females, and is associated with abnormalities in fetal gender with bifid clitoris or penis or with epispadia. Bladder exstrophy can be isolated or can be part of cloacal malformation, as discussed in detail in Chapter 12. The diagnosis of isolated cases of bladder exstrophy can be easily missed on ultrasound. As reported in a literature review of 10 cases, typical clues to the presence of bladder exstrophy include a nonvisible fetal bladder during the first trimester ultrasound 30 examination, along with the presence of normal kidneys and low umbilical cord insertion. In the presence of bladder exstrophy, axial plane of the pelvis in color Doppler will show an absent bladder along with the presence of a “mass of tissue,” resulting from bladder exteriorization. The presence of other fluid-filled structures in the pelvis, including urachal remnant, may be misleading in 31 cases of bladder exstrophy. During the first trimester ultrasound, the diagnosis of bladder exstrophy can be easily missed if imaging of the lower anterior wall of the abdomen and the bladder with the surrounding umbilical arteries is not performed. Bladder exstrophy is a sporadic anomaly, which could be part of syndromic conditions and other more complex 30,31 malformations, thus making fetal counseling difficult, especially in the first trimester. We recommend a close follow-up ultrasound examination at 16 weeks of gestation if the diagnosis of bladder exstrophy is suspected in the first trimester. This is important to confirm the diagnosis and to exclude additional urogenital, gastrointestinal, and other anomalies. The bladder could not be visualized in fetus B during the detailed ultrasound examination. When compared with the normal fetus A, note the presence of a low abdominal cord insertion (short arrow) in B. Also note the presence of irregular tissue inferior to the cord insertion in B, which represents bladder exstrophy. Cloacal abnormalities refer to a spectrum of anomalies where the gastrointestinal, urinary, and genital tracts share a common cavity for discharge. Embryologically, a cloaca persists beyond the fourth to sixth week of gestation when the partition of the cloaca into the urogenital sinus and the rectum fails to occur. The diagnosis of cloacal abnormalities is possible in the first trimester, especially in its severe forms. The presence of a cystic structure in the mid or lower abdomen in the first trimester should alert for the possible presence of cloacal abnormalities, because the cystic structure may represent a communication between the bladder and bowel (Figs. Abnormal Genitalia There are currently no comprehensive studies or reports on the diagnosis of abnormal genitalia in the first trimester. As described earlier in this chapter, the reliable assessment of the normal genitalia can be achieved from 12 weeks onward in optimal imaging. It is, however, difficult to achieve a definitive diagnosis on any gender malformation in the first trimester, with the exception of cloacal abnormalities. Once a renal malformation is suspected in the first trimester, however, ultrasound assessment of the genitalia should be performed because this may help in confirming the diagnosis. The absence of one kidney, in combination with a single umbilical artery and abnormal genitalia, may raise the suspicion for a syndromic condition. Gender discrepancy between chorionic villous sampling and ultrasound in a male fetus could suspect the presence of sexual reversal, as in Smith–Lemli–Opitz syndrome, campomelic dysplasia, chodrodysplasia punctata, and others. Abnormal Adrenal Gland the adrenal gland appears as an anechoic structure between the kidney and diaphragm, with an 5,18 adrenal length about half the length of the kidney. In the second and third trimester of pregnancy, the adrenal glands are commonly abnormal in association with neuroblastoma or hemorrhage, conditions that are not existent in the first trimester. On the other hand, a flat adrenal gland can be a marker for the presence of an empty renal fossa (Figs.
Order levitra without a prescription. City Council 5:14:18.